Date - OMéDIT Haute

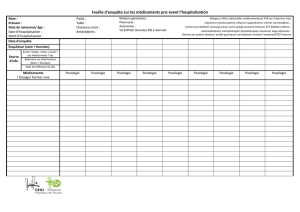
DECLARATION DES EVENEMENTS INDESIRABLES, Y COMPRIS INFECTIEUX
(INFECTIONS PYOGENES OU OPPORTUNISTES), NECESSITANT L'INTERVENTION DU
CLINICIEN CHEZ LES PATIENTS TRAITES PAR MABTHERA
A Contacter : Pharmacovigilance : Tel : 0232889079 Fax : 0232889049 E- Mail : na[email protected]
Praticien déclarant
Nom : E-mail :
Prénom : Tél. :
Date
Identité du Patient
Nom : Prénom :
Sexe : Féminin Masculin Poids : Taille : Date de naissance :
Antécédents :
TRAITEMENT ACTUEL DU PATIENT
◊ MABTHERA :
Indication :
Date de début TTT
Date de Fin
Posologie
rythme
N°cure
Dernière administration
Lot
Heure début
Heure fin
◊ Co-traitement
Immunomodulateurs
en cours ou arrêt
depuis moins de 6
mois
Posologie
Début du
traitement
Date d'arrêt (oui/non)
poursuivi
poursuivi
En cours
Posologie
Début du
traitement
Date d'arrêt (oui/non)
Indication
Cachet :

DECLARATION DES EVENEMENTS INDESIRABLES, Y COMPRIS INFECTIEUX
(INFECTIONS PYOGENES OU OPPORTUNISTES), NECESSITANT L'INTERVENTION DU
CLINICIEN CHEZ LES PATIENTS TRAITES PAR MABTHERA
A Contacter : Pharmacovigilance : Tel : 0232889079 Fax : 0232889049 E- Mail : na[email protected]
EFFETS INDESIRABLES
Date de survenue
Gravité
Inattendu
Evolution
Hospitalisation ou prolongation d'hospitalisation
Service :
Unité :
Incapacité ou invalidité permanente ou durable
Mise en jeu du pronostic vital
Décès
Malformations congénitales
" Non mentionné dans le résumé
caractéristique produit ( RCP)
dans :
son type,
sa gravité,
sa fréquence"
favorable
défavorable
Date de fin éventuelle de l'effet
indésirable :
DESCRIPTION DE L' EVENEMENT INDESIRABLE, Y COMPRIS INFECTIEUX (INFECTIONS
PYOGENES OU OPPORTUNISTES)
(clinique, résultats des explorations réalisées…)
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
........................................................................................................
Examen(s) complémentaire(s) : OUI NON
1
/
2
100%