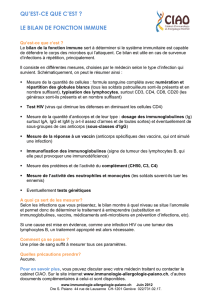
Le rôle des cellules dendritiques

Le rôle des cellules dendritiques
population hétérogène, origine mal connu
DC-SIGN
CCR7
Dec 205
ICAM-1
LFA-3
CMH
Classe II
CMH
Classe I LFA-1
CR4
Cellules dendritiques immatures
Tissus périphériques Cellules dendritiques
Tissus lymphoides
ICAM-2
ICAM-1
LFA-3
B7.1
CMH
Classe II
CMH
Classe I
DC-SIGN
B7.2
LFA-1
DC-CK

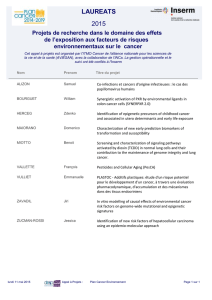
Molécules associées aux DC
Langerine lectine +++ formation de granules de birbeck
Dectine -2 lectine +++ ingestion ag
DC-SIGN lectine +++ interaction avec cellules T/ ICAM-3
DC-LAMP glycoprotéine lysosomale +++ présentation ag
DEC-205 lectine +++ ingestion ag
DC-CKI chimiokine +++ attraction cellules T naives
TARC chimiokine ++ attraction lymphocytes memoires act.
MDC chimiokine + attraction lymphocytes memoires act.

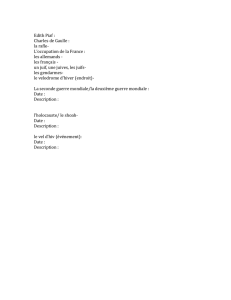
Les populations de DC
DCs myéloides : de monocytes (in vitro, GM-CSF)
Dcs lymphoides : voie thymique , expression CD8 (TCR-)
Cellules plasmacytoides : Dc immature,
origine lymphoide ou myéloide ?
CD11c-, secrètent IFN-α,
dépendants d ’IL-3 mais pas GM-CSF
pour Dc matures
DC1 (TH1) ?
Multifonctionnel ? DC2 (TH2) ?
Fonction limitée ?

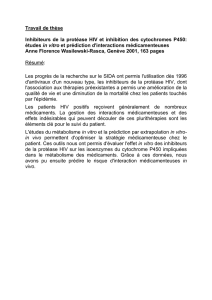
Les populations de DC
DC du sang : précurseurs CD11c+
précurseurs CD14-CD1+ GM-CSF+ TNF-α
DC épithéliales (cellules Langerhans) : uniquement épithélium
Fcγet Fc ε, CD1a, Langerin (migration, ingest. Ag)
DC interstitales : CD68 , pas de marqueurs LC
DC monocytaires : GM-CSF + IL-4
DC centre germinal ganglion : CD11c+, CD4+, CD3-, stim. CD4+
DC plasmocytoides (DC2) : dépendants de IL-3, CD11c-, CXCR3

Origine des
cellules
dendritiques
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
1
/
37
100%

![Pene_GrrrOH_02072015 - public [Mode de compatibilité]](http://s1.studylibfr.com/store/data/001230682_1-f593ab7310c23a44db266019e9363fd7-300x300.png)
![Poster CIMNA journée CHOISIR [PPT - 8 Mo ]](http://s1.studylibfr.com/store/data/003496163_1-211ccc570e9e2c72f5d6b6c5d46b9530-300x300.png)