objective - Canceropole Grand ouest

ROMANCE
ESSAI D'ABSTENTION DE RADIOTHÉRAPIE MAMMAIRE DANS
LES CARCINOMES CANALAIRES IN SITU DU SEIN À FAIBLE
RISQUE DE RÉCIDIVE, APRÈS CHIRURGIE CONSERVATRICE
A. FOURQUET

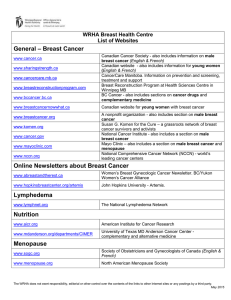
Femmes ≥ 55 ans, ménopausées
Carcinome canalaire in situ strict,
confirmé
CCIS découvert incidemment sur biopsie
ou chirurgie d’une lésion bénigne
Grade nucléaire bas ou intermédiaire
Microcalcifications mammographiques
Unifocalité confirmée par IRM
Chirurgie conservatrice
Berges saines d’emblée (≥ 2 mm), ou
après ré-excision
pT < 25 mm
Pas de microcalcifications résiduelles sur
une mammographie post-opératoire
Profil IHC confirmé par évaluation
centralisée, associant:
RO ≥ 10 %
RP ≥ 10 %
ERBB2 – (confirmé par FISH si douteux)
KI67 < 15%
Eligibility Criteria
Age < 55 ans
Prédisposition génétique
Tumeur palpable, opacité, écoulement
mamelonnaire sanglant
Multifocalité
Berges atteintes
Cancer microinvasif ou invasif associé
Grade nucléaire élevé
Microcalcifications résiduelles
Traitement endocrinien programmé
INCLUSION EXCLUSION

Objectives
PRIMARY OBJECTIVE
Déterminer si une utilisation combinée de marqueurs cliniques,
histologiques et immunohistochimiques peut identifier un groupe
de patientes à très faible risque de récidive locale, pour lesquelles
une radiothérapie du sein après chirurgie conservatrice pourrait
être omise
SECONDARY OBJECTIVES
Pronostic des récidives locales
Evaluation des séquelles et du résultat esthétique
Mesure de la qualité de vie
Valeur pronostique des TIL dans les CCIS
Validation d’une signature génomique prédictive
Analyse médico-économique

Schéma de l’étude
323 patients dans chaque bras (700 au total), 3 ans d’inclusion, 10 ans de suivi

LORD
LOW RISK DCIS
R. ROUZIER
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
1
/
32
100%