Art therapy among palliative cancer patients: Aesthetic dimensions

Art therapy among palliative cancer patients:
Aesthetic dimensions and impacts on symptoms
CE
´DRIC LEFE
`VRE, PH.D., MATHILDE LEDOUX, M.D., AND MARILE
`NE FILBET, M.D.
1
Centre de Soins Palliatifs, Centre Hospitalier Lyon-Sud, Hospices Civils de Lyon, Pierre-Be
´nite, France
(RECEIVED March 17, 2015; ACCEPTED July 6, 2015)
ABSTRACT
Objective: This study aimed to explore whether aesthetic beauty and the pleasure that results
from artistic activity can contribute to a reduction in the symptoms experienced by palliative
care patients, and to improve the effectiveness of art therapy sessions.
Method: A self-assessment of six symptoms (pain, anxiety, ill-being, tiredness, sadness, and
depression) adapted from the Edmonton Symptom Assessment System (ESAS) was completed by
patients before and after a one-hour art therapy session. This assessment was completed after the
session with a self-assessment of aesthetic feeling. A correlation analysis was then performed.
Results: From July of 2012 to December of 2013, 28 patients took part in 63 art therapy
sessions. On the whole, these sessions reduced the global distress of patients by 47%
(p,0.0001). There was a significant reduction in all the symptoms studied; pain ( p¼0.003),
anxiety ( p,0.0001), ill-being ( p,0.0001), tiredness ( p,0.0001), sadness ( p,0.0001), and
depression ( p,0.0001). A study of the significant correlations (0.35 ,rs ,0.52, p,0.05)
indicated that technical satisfaction, aesthetic beauty, and pleasure are all involved to varying
degrees in reduction of symptoms.
Significance of results: Our findings confirm the benefits of art therapy in reducing distress
within the palliative context. We also make suggestions for the future direction and
improvement of these sessions.
KEYWORDS: Art therapy, Palliative care, Cancer, Symptoms, Aesthetic
INTRODUCTION
Increasing numbers of patients with cancer use com-
plementary therapies in order to improve their qual-
ity of life (Horneber et al., 2012; Klafke et al., 2012).
Art therapy can be defined as “the exploitation of the
artistic potential of a person with a humanitarian
and therapeutic goal” (Forestier, 2009). It includes
the patient’s characteristics as well as the physical
and psychological dimensions of their distress. This
is one of the reasons why this type of therapy has
been employed with greater frequency over the past
two decades (Wood et al., 2011; Geue et al., 2010).
The scientific literature contains a large number of
studies on the effectiveness of art therapy for symptom
reduction (Nainis et al., 2006;Rhondalietal.,2013)and
as a coping mechanism that enhances the well-being
(Bar-Sela et al., 2007;Forzonietal.,2010;Linetal.,
2012; Oster et al., 2006;Thymeetal.,2009)ofpatients
with cancer.
During a session, three dimensions of the aesthetic
feeling, self-assessed by the patient, can contribute
to the effect of the art therapy (Forestier, 2009;
2004): the GOOD, which is associated with the plea-
sure the patient experiences while doing the activity
and his/her desire to continue that activity; the
WELL, which is associated with the technical satisfac-
tion with creating something; and the BEAUTIFUL,
which is associated with the aesthetic satisfaction ach-
ieved when carrying out the work.
These three dimensions are the basis for the “har-
monic cube,” a self-assessment tool that has been de-
veloped over the past 12 years by the school of art
therapy in Tours (Forestier, 2009;2004). These
Address correspondence and reprint request to: Marile
`ne Fil-
bet, Centre de Soins Palliatifs, Centre Hospitalier Lyon-Sud, Hos-
pices Civils de Lyon, 165 Chemin du Grand Revoyet, 69310
Pierre-Be
´nite, France. E-mail: marilene.filbet@chu-lyon.fr.
Palliative and Supportive Care (2015), 0, 1–5.
#Cambridge University Press, 2015 1478-9515/15
doi:10.1017/S1478951515001017
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
PAX 15-101
1

dimensions are a means for analyzing the complex of
feelings involved in an art therapy session.
Our self-assessment tool has two objectives: (1) to
provide a frame within which to measure how the pa-
tient’s aesthetic taste evolves, and (2) to allow the pa-
tient to self-assess their work in each consecutive
session.
The purpose of our study, based on self-assessment
by patients of their aesthetic experience, was to look
at the impact of one or more art therapy sessions on
the symptoms (pain, anxiety, ill-being, sadness, and
depression) of inpatients in a palliative care unit.
METHOD
Recruited Patients
The patients were gradually recruited from an acute
palliative care unit over a period of 18 months.
Among the inclusion criteria were an advanced can-
cer diagnosis, the ability to communicate in French,
an ability to take part in an hour-long art therapy
session, and the ability to complete all the self-as-
sessments. Some 28 patients were recruited (21 wom-
en and 7 men) for a total of 63 art therapy sessions.
Intervention in Art Therapy
Patients took part in at least one session facilitated
by a qualified art therapist. Several days before the
session, each patient was invited to choose his/her
preferred medium of artwork. The choice of tech-
nique and subject depended mainly on the patient’s
preferences and physical abilities to produce some-
thing that was meaningful for them. Different art
techniques were employed: painting, drawing, pho-
tography, modeling, and sculpture. The session could
take place in the patient’s room or in a studio outside
the unit, depending on the patient’s wishes and their
physical abilities. The art therapist focused primari-
ly on the technical aspect of the artwork. Depending
on the project and the length of the stay of the pa-
tient, from 1 to 10 hour-long session(s) were offered.
Symptom Assessment Procedure
The Edmonton Symptom Assessment System
(ESAS) is a self-assessment tool that allows patients
to document the intensity of nine frequently occur-
ring symptoms (pain, nausea, tiredness, drowsiness,
loss of appetite, dyspnea, depression, anxiety, and
feelings of ill-being) using a visual scale ranging
from 0 (no symptom) to 10 (worst symptom). Use of
the ESAS for patients with cancer has shown good
test–retest reliability (Bruera et al., 1991;1989;
Chang et al., 2000; Richardson & Jones, 2009). We
used a modified ESAS to assess the physical and psy-
chological distress of our patients. Our self-assess-
ment tool excluded four symptoms that were not
sensitive to art therapy according to various studies
(Nainis et al., 2006; Rhondali et al., 2013): nausea,
drowsiness, loss of appetite, and dyspnea. We added
the “sadness” symptom. Although sadness is not a
validated symptom for the ESAS, it seemed more rel-
evant to assess sadness and depression, since depres-
sion cannot be relieved in such a short amount of time.
Patients were invited to complete the modified
ESAS five minutes before and five minutes after
each session.
Aesthetic Dimensions Assessment
Using the same type of visual scale, three dimen-
sions—the GOOD, the WELL, and the BEAUTI-
FUL—were self-assessed by patients five minutes
after the session based on the “harmonic cube” (For-
estier, 2009;2004) model, developed in France. In re-
spect of GOOD, 0 corresponds to “a lot of pleasure”
and 10 to “no pleasure at all.” With respect to WELL,
0 corresponds to “very well done” and 10 to “done
badly.” As for BEAUTIFUL, 0 corresponds to “I like
it a lot” and 10 to “I don’t like it.”
Data Analysis
Statistical analyses were carried out with R 2014
software for Mac (R Core Team, 2014).
We employed nonparametric statistical tests in or-
der to eliminate an hypothesis based on our sampling
distribution. The Wilcoxon test for paired samples
was used to compare data for variables before and af-
ter an intervention. The Mann–Whitney test was
utilized to compare the effect of the first session on
the symptoms and three dimensions of the aesthetic.
A Friedman test was also used to compare the three
dimensions of the aesthetic. Links between the vari-
ables were studied by means of the correlation matrix
of Spearman. We used ClustOfVar, an R package for
clustering our variables.
In all our statistical evaluations, pvalues of 0.05
or less were considered statistically significant.
The study was approved by the ethics committee
and institutional review board of the Hospices Civils
de Lyon.
RESULTS
Of the 28 patients recruited, 22 were included in the
analysis, for a total of 53 art therapy sessions. Six
patients were excluded because of incomplete self-
assessment.
Lefe
`vre et al.2
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
PAX 15-101

Patient Characteristics
Of the 22 total patients, 16 were women and 6 men
(see Table 1). The median age at baseline was 56.5
years, and the median time until death was 43
days, with an exception of 5 patients still living.
The diagnoses were split between hematological,
breast, head and neck, gastrointestinal, lung, uro-
logical, and other cancers. Across all our results,
the two genders did not show any significant
difference.
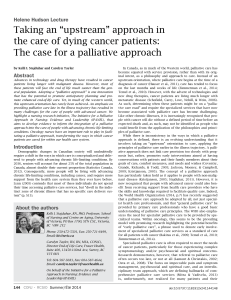
The Symptoms
The hour-long art therapy session had a significant
effect on global distress (sum of the six symptoms)
and on each individual symptom (Figure 1). Global
distress was on average reduced by 47% ( p,
0.0001). During 53 sessions, only 1 produced an in-
creased distress by 12.3%. Taken individually, the re-
duction in symptoms strongly varied from one person
to another. On average, the standard deviation for
the percentage of reduction was 60.8%.
Before a session, the self-assessed scores for sad-
ness and depression were not significantly different
(p¼0.407) and were the more strongly correlated
of all the symptoms (rs ¼0.9). After a session, the
scores for sadness and depression were significantly
different at risk (
a
¼8%), with a very slight inflexion
of the correlation (rs ¼0.88). The strongest correla-
tion after a session was observed between depression
and anxiety (rs ¼0.89).
We noted that all the symptoms before the session
were all significantly correlated with each other
(0.28 ,rs ,0.90, p,0.05). This situation was the
same after a session (0.41 ,rs ,0.89, p,0.05),
with an average correlation rate significantly higher
than the one obtained before the session ( p¼0.002).
The Effect of the First Session
The effects on global distress and individual symp-
toms for the first and subsequent sessions were not
significantly different ( p0.2). The effect of an art
therapy session on symptoms did not depend on the
number of sessions.
The Three Dimensions of the Aesthetic
Self-assessment of the three dimensions of the aes-
thetic after a session revealed significant differences
(p¼0.0003). On average, the score for GOOD was
higher than that for BEAUTIFUL, which in turn
was higher than that for WELL. The standard devia-
tions followed an opposite order.
The GOOD, the WELL and the BEAUTIFUL were
linked by significant correlation rates higher than
rs ¼0.6.
The aesthetic experience was significantly greater
for sessions following the first session for the WELL
(p¼0.008) and the BEAUTIFUL ( p¼0.004). It
was significantly greater for the first session for the
GOOD ( p¼0.039).
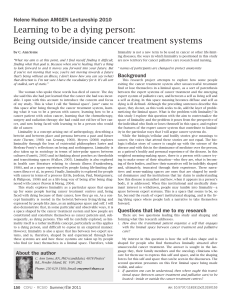
Symptoms and the Three Dimensions of the
Aesthetic
Our analysis of the Spearman correlations matrix
(Table 2) indicates that the dimension of the GOOD
(pleasure felt by the patient) was significantly corre-
lated ( p,0.05) with the percentage of reduction in
global distress. The dimensions of the GOOD and
the WELL (a feeling of having done things correctly)
were both correlated to the percentage reduction in
pain, anxiety, and ill-being ( p,0.05). The dimen-
sion of the WELL was also correlated with the per-
centage reduction in sadness and depression ( p,
0.05). The dimension of the BEAUTIFUL was corre-
lated with the percentage reduction in pain ( p,
0.05).
Table 1. Patient characteristics
Characteristics n%
Age (median +SD, range,
in years)
56.5 +10.7 (30–85)
Gender
Female 16 73
Male 6 27
Cancer diagnosis
Hematological 6 27
Breast 4 18
Head and neck 3 14
Gastrointestinal 3 14
Lung 2 9
Urological 2 9
Other cancer 2 9
Time until death (median +SD,
range, in days)
43 +138 (3–?)
Fig. 1 - B/W online
Fig. 1. Impact of an art therapy session on symptoms.
Art therapy among palliative cancer patients 3
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
PAX 15-101

The cluster analysis carried out with the ClustOf-
Var R package confirmed the data correlations. We
found that GOOD was very closely associated with
reduction in anxiety and ill-being, WELL showed a
very close relationship with reduction in anxiety,
while BEAUTIFUL was associated with reduction
in pain.
DISCUSSION
According to previously available studies, art thera-
py sessions mainly focus on the fine arts, last about
an hour and a half, and reduce almost by half
(247%) the symptomatology of patients with cancer
(Nainis et al., 2006; Rhondali et al., 2013). Even the
experience of tiredness, which is the most prevalent
of symptoms (average ¼3.9), reduces on average by
36% after a person is stimulated for an hour, illustrat-
ing the physical and psychological impact of sessions.
From a neurophysiological point of view, this benefi-
cial impact can partly be explained by the pleasure
the patients experience and self-assess. Numerous
studies have revealed that the “aesthetic emotion”
that a patient feels after having listened “actively”
to music activates dopaminergic circuits (Archie
et al., 2013; Zatorre & Salimpoor, 2013). Further-
more, if a musical activity takes place, the brain re-
leases endorphins (Dunbar et al., 2012). Some
correlations could even suggest some comparable
neurobiological effects gained from the practice of
fine arts. The correlations between pleasure experi-
enced (GOOD) and global distress reduction, as
well as between aesthetic emotion (BEAUTIFUL)
and pain reduction, seem to underline the same
fact. The fact that distress, particularly the experi-
ence of pain (Chardon, 2010), is quickly reduced
(within less than an hour), but for short periods of
time (less than 12 hours), seems to be compatible
with this neurophysiological hypothesis.
We can infer a psychological explanation that is re-
lated to self-confidence and to a feeling of existing in-
dependently from the status of an ill person. The
dimension of the WELL self-assessed by patients is
related in a more or less complex way to their self-
confidence (Forestier, 2009;2004;2007). The more a
patient feels satisfied with their work, the more
they will feel confident of succeeding again in the fu-
ture. We noted that this dimension of the WELL is re-
lated in particular to anxiety reduction. The feeling
of mastering an artistic technique, even a small
one, could result in improved self-confidence and de-
creased anxiety. The fact that the self-assessed
WELL item improved after the first session indeed
seems to indicate a positive effect on self-confidence.
Studies in the literature dedicated to art therapy
omit this dimension of the WELL. Yet it appears
that it could play a role in providing a therapeutic ef-
fect. Artistic technique is a very important element
when considering art therapy, particularly in a palli-
ative situation, where time is limited. Instead of be-
ing cared for in a passive way, the patient is able to
take a more active role during art therapy. This in
turn changes the attitude of family members and pro-
fessional carers, who no longer perceive the patient
as a “person with cancer” (Wood et al., 2011). The
feeling of existing, of being able to do and succeed,
could thus contribute to improved symptoms.
We can assume that a patient who enjoyed a ses-
sion and is aware of the implications of the self-
assessment before and after the session might
conform to the expectations of the art therapist,
that is, to overassess the positive impact of the ses-
sion, after their first experience of one. The absence
of a significant difference between the first and fol-
lowing sessions is a good indicator that leads us to as-
sume that those assessment biases are not too
significant. We could also have expected that the ini-
tial distress, in the context of various sessions, would
be reduced by an anticipatory effect. The data reveal
no significant difference in level of initial distress.
This anticipatory effect and its positive effect on pa-
tients could partly be concealed by a quick deteriora-
tion of the patient’s health. For the therapist, a single
session seems as therapeutic on the symptomatic level
as a greater number of sessions. In palliative care
patients, where time is short, it could be appropriate
to suggest an art therapy session at any stage, even
at the end of life.
The art therapy session and its positive effects on
well-being could also have an effect on better identi-
fication of feelings, as the data relative to pain and
Table 2. Correlations matrix (Spearman) of the three
dimensions of the aesthetic and symptomatic reduc-
tions
GOOD WELL BEAUTIFUL
Pain (% reduction) 20.374* 20.456* 20.517*
Anxiety
(% reduction)
20.454* 20.470* 20.279
Feeling of ill-being
(% reduction)
20.471* 20.308* 20.263
Tiredness
(% reduction)
20.186 0.019 0.000
Sadness
(% reduction)
20.198 20.399* 20.163
Depression
(% reduction)
20.288 20.393* 20.170
Total distress
(% reduction)
20.352* 20.287 20.222
*p,0.05.
Lefe
`vre et al.
4
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
PAX 15-101

sadness suggest, those two symptoms being the most
importantly correlated before sessions (rs ¼0.9). Be-
fore a session, self-assessments of sadness and de-
pression were identical ( p¼0.407), whereas they
were different after at the risk (
a
¼8%, p¼0.076).
If this hypothesis were proved correct, art therapy
could prove to be a useful tool in palliative care, par-
ticularly when patients have to make important deci-
sions requiring self-awareness of their situation.
Given the limitations of this work owing to the
number of participants (53 sessions and 22 patients),
the absence of a control group, and its monocentric
nature, generalization of our results cannot be as-
sured. However, the great statistical significance of
symptomatic benefits after an art therapy session in-
dicates and confirms very encouraging tendencies for
patients and nursing staff. The “harmonic cube”
model seems to be interesting and innovative in re-
search and could contribute to better comprehension
of the internal processes involved in art therapy.
These results are an incentive for us to pursue fur-
ther studies about the effectiveness of art therapy
that would involve a larger number of participants
with control groups and at many different centers.
ACKNOWLEDGMENTS
The authors wish to thank Avril Jackson and Le
´a Monsar-
rat for their translation and proofreading.
REFERENCES
Archie, P., Bruera, E. & Cohen, L. (2013). Music-based in-
terventions in palliative cancer care: A review of quanti-
tative studies and neurobiological literature. Supportive
Care in Cancer,21(9), 2609–2624.
Bar-Sela, G., Atid, L., Danos, S., et al. (2007). Art therapy
improved depression and influenced fatigue levels in
cancer patients on chemotherapy. Psycho-Oncology,
16(11), 980 –984.
Bruera, E., MacMillan, K., Hanson, J., et al. (1989) The Ed-
monton staging system for cancer pain: Preliminary
report. Pain,37(2), 203–209.
Bruera, E., Kuehn, N., Miller, M.J., et al. (1991). The Ed-
monton Symptom Assessment System (ESAS): A simple
method for the assessment of palliative care patients.
Journal of Palliative Care,7(2), 6–9.
Chang, V.T., Hwang, S.S. & Feuerman, M. (2000). Validation
of the Edmonton Symptom Assessment Scale. Cancer,
88(9), 2164–2171.
Chardon, F. (2010). Les spe
´cificite
´s de l’art-the
´rapie en
oncologie me
´dicale lors de l’accompagnement en fin de
vie. In Profession: Art-the
´rapeute. R. Forestier (ed.),
pp. 75–78. Paris: Elsevier –Masson.
Dunbar, R.I., Kaskatis, K., MacDonald, I., et al. (2012). Per-
formance of music elevates pain threshold and positive
affect: Implications for the evolutionary function of mu-
sic during interventional radiological procedures, effect
on sedation, pain and anxiety: A randomised controlled
trial. Evolutionary Psychology,10(4), 688–702.
Forestier, R. (2004). Tout savoir sur l’art occidental. Lau-
sanne, Paris: Favre.
Forestier, R. (2007). L’e
´valuation en art-the
´rapie: Pratiques
internationales. Paris: Elsevier–Masson.
Forestier, R. (2009) Tout savoir sur l’art-the
´rapie. Lau-
sanne: E
´dition Favre.
Forzoni, S., Perez, M., Martignetti, A., et al. (2010). Art
therapy with cancer patients during chemotherapy ses-
sions: An analysis of the patients’ perception of helpful-
ness. Palliative & Supportive Care,8(1), 41– 48.
Geue, K., Goetze, H., Buttstaedt, M., et al. (2010). An over-
view of art therapy interventions for cancer patients and
the results of research. Complementary Therapies in
Medicine,18(3–4), 160–170.
Horneber, M., Bueschel, G., Dennert, G., et al. (2012). How
many cancer patients use complementary and alterna-
tive medicine: A systematic review and metaanalysis.
Integrative Cancer Therapies,11(3), 187–203.
Klafke, N., Eliott, J.A., Wittert, G.A., et al. (2012). Preva-
lence and predictors of complementary and alternative
medicine (CAM) use by men in Australian cancer outpa-
tient services. Annals of Oncology,23(6), 1571– 1578.
Lin, M.H., Moh, S.L., Kuo, Y.C., (2012). Art therapy for ter-
minal cancer patients in a hospice palliative care unit in
Taiwan. Palliative & Supportive Care,10(1), 51–57.
Nainis, N., Paice, J.A., Ratner, J., et al. (2006). Relieving
symptoms in cancer: Innovative use of art therapy. Jour-
nal of Pain and Symptom Management,31(2), 162–169.
Oster, I., Svensk, A., Magnusson, E., et al. (2006). Art ther-
apy improves coping resources: A randomized, con-
trolled study among women. Palliative & Supportive
Care,4(1), 57–64.
R Core Team (2014). R: A language and environment for
statistical computing. Vienna, Austria: R Foundation
for Statistical Computing. Available at http://www.R-
project.org/.
Rhondali, W., Lasserre, E. & Filbet, M. (2013). Art therapy
among palliative care inpatients with advanced cancer.
Palliative Medicine,27(6), 571–572.
Richardson, L.A. & Jones, G.W. (2009). A review of the re-
liability and validity of the Edmonton Symptom Assess-
ment System. Current Oncology,16(1), 55.
Thyme, K.E., Sundin, E.C., Wiberg, B., et al. (2009). Indi-
vidual brief art therapy can be helpful for women with
breast cancer: A randomized controlled clinical study.
Palliative & Supportive Care,7(1), 87–95.
Wood, M.J., Molassiotis, A. & Payne, S. (2011). What re-
search evidence is there for the use of art therapy in
the management of symptoms in adults with cancer?
A systematic review. Psycho-Oncology,20(2), 135– 145.
Zatorre, R.J. & Salimpoor, V.N. (2013). From perception to
pleasure: Music and its neural substrates. Proceedings
of the National Academy of Sciences of the United States
of America,110(Suppl. 2), 10430 –10437.
Art therapy among palliative cancer patients 5
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
PAX 15-101
1
/
5
100%