FEA TUR ES /R

357
CANADIAN ONCOLOGY NURSING JOURNAL � VOLUME 25, ISSUE 3, SUMMER 2015
REVUE CANADIENNE DE SOINS INFIRMIERS EN ONCOLOGIE
FEATURES/RUBRIQUES
ABstrAct
Family members have multiple roles when
caring for someone diagnosed with can-
cer. The burden associated with these roles
can result in family members experienc-
ing elevated levels of emotional distress
including depression, anxiety, and physical
complaints. For comprehensive psychoso-
cial care to be all inclusive, the well-being
and distress levels of family members must
also be addressed. To date, little is known
about the speci c sources of distress for
family members.
The purpose of this research study was
to ll this gap. Speci cally, the researchers
developed a unique screening tool to iden-
tify sources contributing to family mem-
bers’ emotional distress. The study was
conducted in three phases: 1) a compre-
hensive literature review was done to elicit
a rst set of items, 2) two separate focus
groups of health care professionals and
family members were held to obtain their
feedback on possible items that would com-
prise the tool and, 3) a sample of family
members was invited to speak to the rele-
vancy of the proposed items. Results from
these analyses led to a tool comprising 46
items. Family member responses on these
items suggested that they are often con-
fronted with unique sources of distress
including those related to self-care, patient
care, and relational.
Cancer a ects the entire family.
While emotional distress experi-
enced by cancer patients is widely
studied (Graves et al., 2007; McLean
& Jones, 2007; Sellick & Edwardson,
2006; Zabora, BrintzenhofeSzoc,
Curbow, Hooker, & Piantados, 2001),
the distress of the family members is
often overlooked. Yet, the rates of dis-
tress experienced by family members
of oncology patients have been shown
to be elevated. For instance, using
the Distress Thermometer, a team of
researchers reported that 29.2% and
18% of family members of oncology
patients experienced moderate and high
levels of distress respectively (Zwahlen,
Hagenbuch, Carley, Recklitis, & Buchi,
2008).
Additionally, research suggests that
family members’ distress tends to
increase during speci c time points
across the disease trajectory (Murray
et al., 2010). Finally, a patient’s overall
coping is said to be positively related to
the well-being of the family members
(Northouse, 2012). Based on the
population of family members seen in
our psychosocial oncology program, we
argue that comprehensive patient care
must also take into account addressing
the needs of family members who are
directly involved in the cancer experience
of their loved one. At present, all new
patients and family members who
are seen by a clinician in the program
are invited to complete the Canadian
Problem Checklist (CPC) (Cancer
Journey Action Group, 2009) to help
identify the sources of their distress.
While the CPC was not speci cally
designed for family members, we were
using it to obtain some information on
what they identi ed as sources of distress
for them. Family members had noted
and provided us with feedback that they
felt the tool was not entirely applicable
to them. They felt that not all of their
sources of distress were identi ed, or
they felt the sources of distress listed
were very patient-speci c. In order to
address this concern, we recognized that
the development of a screening tool for
these family members was a necessary
rst step in the provision of optimal care
to these family members.
The purpose of the present study was
to develop a screening tool designed
to identify the distress level of family
members with a list of their speci c con-
cerns. The study was completed in three
phases. First, a comprehensive litera-
ture review was conducted on sources
contributing to emotional distress in
family members. Second, separate
focus groups of health care profession-
als in oncology and family members of
cancer patients were conducted. Goals
of these focus groups were to: 1) review
the preliminary items generated from
the literature review, 2) solicit sugges-
tions of additional or removal of items
and, 3) provide feedback on the Family
BrieF communicAtion
Comprehensive psychosocial care of cancer
patients: Screening for distress in family members
by Anita Mehta and Marc Hamel
ABout tHe AutHors
Anita Mehta, RN, PhD, Clinical Nurse Specialist and Co-Director, McGill University
Health Centre, Montreal, QC
Marc Hamel, PhD, Clinical Director, Psychosocial Oncology Program, McGill
University Health Centre, Montreal, QC
Correspondence: Anita Mehta, 1650 Cedar Avenue T6-301, Montreal, QC
Tel: 514 934-1934 ext 44815; Fax: 514 934-8593; Email: [email protected]
FundinG AcKnoWledGement
The Nursing Research Development Fund, with the generous support of the Newton Foundation and
matching funds provided by the Montreal General Hospital, Royal Victoria Hospital and Montreal Children’s
Hospital Foundations (McGill University Health Centre).

358 Volume 25, Issue 3, summer 2015 • CanadIan onCology nursIng Journal
reVue CanadIenne de soIns InfIrmIers en onCologIe
FEATURES/RUbRiqUES
Member Problem Checklist (FMPC).
These focus groups were audio-taped
and transcribed. The content of these
groups were coded and relevant themes
were extracted. Finally, a sample of
N=106 family members recruited from
oncology clinics were asked to rate the
relevancy of the FMPC items to their
overall experience.
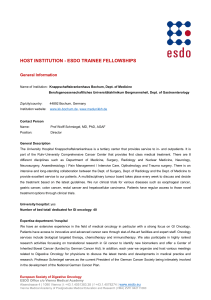
The screening tool resulted in 46
items (see Figure 1). The results of
this research indicated that, like can-
cer patients, family members reported
sources of distress related to practi-
cal (e.g., transportation/parking), emo-
tional (e.g., anxiety/worry), social/
family (e.g., lack of support), informa-
tional (e.g., about prognosis) and spir-
itual domains (e.g., faith). However,
family members also reported unique
sources of distress relevant to them
including those related to relational
(e.g., relationship with the patient),
self-care (e.g., managing one’s own
time) and patient-care (e.g., managing
patient’s symptoms).
The study also asked participants to
respond to qualitative questions pertain-
ing to their experience in completing
the screening items. Many felt strongly
that the new “checklist covers most con-
cerns a family member might have” and
that it was “clear” and “easy to read.”
The average time of completion was 7.6
minutes and a range of time needed to
complete the FMPC, from 30 seconds to
20 minutes was noted by reading their
qualitative responses. These responses
on the qualitative questions suggested
that the FMPC was easy for them to
complete and they found to be a mean-
ingful tool for them.
Family members are often consid-
ered the “hidden patient” in oncology
settings. They are often required to
deliver dierent types of care to patients,
without any former training and recog-
nition, and are expected to be continu-
ously supportive during the patient’s
illness. As a result, family members can
become easily overwhelmed, anxious
and/or depressed. The development of
this clinical tool specically designed to
screen for the sources of distress expe-
rienced by family members is the rst
step towards a more comprehensive
assessment of their distress and, likely,
that of the patient. This assessment/
screening places nurses, and all health
care professionals, in a stronger posi-
tion to provide optimal support and
appropriate family interventions in the
future.
reFerences
Cancer Journey Action Group (2009). Guide
to implementing screening for distress, the
6th vital sign: Moving towards person-
centered care. Retrieved from www.
canadianpartnershipagainstcancer.ca
Graves, K.D., Arnold, S.M., Love, C.L.,
Kirsh, K.L, Moore, P.G., & Passik,
S.D. (2007). Distress screening in a
multidisciplinary lung cancer clinic:
Prevalence and predictors of clinically
signicant distress. Lung Cancer, 55(2),
215–224.
McLean, L.M., & Jones, J.M. (2007). A
review of distress and its management in
couples facing end-of-life cancer. Psycho-
Oncology, 16(7), 603–617.
Murray, S.A., Kendall, M., Boyd, K., Grant,
L., Highet, G., & Sheikh, A. (2010).
Archetypal trajectories of social,
psychological, and spiritual wellbeing
and distress in family care givers of
patients with lung cancer: Secondary
analysis of serial qualitative interviews.
British Medical Journal, 340, 2581.
Northouse, L.L. (2012). Helping patients
and their family caregivers. Oncology
Nursing Forum, 39(5), 500–506.
Sellick, S.M., & Edwardson, A.D. (2006).
Screening new cancer patients for
psychological distress using the hospital
anxiety and depression scale. Psycho-
Oncology, 16(6), 534–542.
Zabora. J., BrintzenhofeSzoc, K., Curbow,
B., Hooker, C., & Piantadosi, S. (2001).
The prevalence of psychological distress
by cancer site. Psycho-Oncology, 10(1),
19–28.
Zwahlen, D., Hagenbuch, N., Carley, M.I.,
Recklitis, C.J., & Buchi, S. (2008).
Screening cancer patients’ families
with the distress thermometer (DT): a
validation study. Psycho-Oncology, 17(10),
959–66.
Figure 1
Family Member Problem Checklist:
Please check all of the following items that
have been a concern or problem for you in the
past week, including today
Practical
Finances
Legal Issues
Transportation/Parking
Household duties
Taking care of others
Work/Studies
Managing my own time
Information
About the disease
About the treatment
About prognosis
About supportive resources
Communication
Acting as a spokesperson
Difficulty talking about certain topics
Emotional
Sadness
Anger/frustration
Anxiety/worry
Guilt
Feeling overwhelmed
Helplessness
Shock
Resentment
Mehta & Hamel, 2015
Social
Feeling alone
Lack of support
Expectations from others
Relational
Change in social roles
Relationship with patient
Relationship with health care team
Family dynamics
Spiritual
Faith
Meaning and purpose
Hope
Death/Dying
Self-Care
Sleep
Appetite
Concentration/Memory
Fatigue/Weakness
Intimacy/Sexuality
My own physical health problems
My own mental health problems
Finding time for myself
Coping
Patient Care
Managing patient symptoms
Managing patient medications
Organising patient appointments
Caring for the patient at home
Self-confidence as a caregiver
1
/
2
100%