Document PPT – 10Mo

CONGRES SFCP 2012
AJACCIO 11.5.2012
ANALYSE CRITIQUE D’ARTICLE
BRUNO CUTULI
INSTITUT DU CANCER COURLANCY - REIMS

EFFECTS OF RADIOTHERAPY AFTER BREAST
CONSERVING SURGERY ON 10-YEAR RECURRENCE
AND 15-YEAR BREAST CANCER DEATH:
META-ANALYSIS OF INDIVIDUAL PATIENT DATA FOR
10801 WOMEN IN 17 RANDOMISED TRIALS
EARLY BREAST CANCER TRIALIST COLLABORATIVE
GROUP (EBCTCG)
LANCET 2011, 378: 1707-1726

CUZICK J et al CANCER TREAT REP 1987, 71: 15-29
CUZICK J et al JCO 1994, 12: 447-453
EBCTCG NEJM 1995, 333: 1444-1455
EBCTCG LANCET 2000, 355: 1757-1770
EBCTCG LANCET 2005, 366: 2087-2186
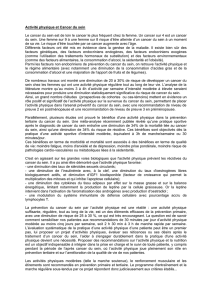
ACTUALISATION DES META-
ANALYSES REALISEES DE 1987 à 2005

du suivi (9 des 10 essais déjà inclus)
Inclusion de 7 nouveaux essais, dont 6 incluant des
patientes « à bas risque » de rechute
Evaluation du risque de rechute à 10 ans en fonction de
différents facteurs pronostics.
Evaluation de la réduction de décès par CS à 15 ans.
Stratification des analyses:
pN0 / pN+; âge (< 40; 40-49; 50-59; 60-69; ≥ 70);
grade (mSBR); pT; ER; TAM
NOUVEAUTES DE CETTE NOUVELLE
ANALYSE:

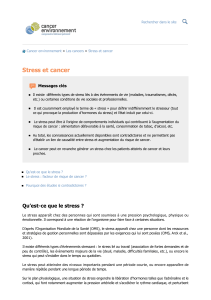
CATEGORIE
ANNEES n DECES
A] LUMPECTOMY
(ORIGINAL
TRIALS)
1976-86 4398
1982 45%
B] SECTOR RESECTION
OR QUADRANTECTOMY
1981-91 2399
708 30%
C] LUMPECTOMY
(LOW
-RISK WOMEN)
1989-99 4004
453 11%
pN
pN0
7287
1801 25%
pN
+1050
585 56%
NP
2464
757 31%
TOTAL
10801 3143
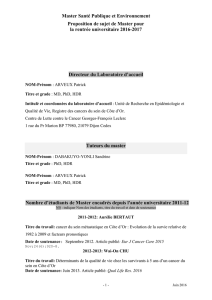
REPARTITION DES ESSAIS:
29%
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
1
/
47
100%