Endocardite, millésime 2016 - Évaluation des présentations

ENDOCARDITE, MILLÉSIME 2016
Véronique Cyr, Cardiologue
CHUM


CONFLIT D’INTÉRÊTS
➤Aucun conflit d’intérêts en lien avec cette présentation.

OBJECTIFS DE LA PRÉSENTATION
➤Connaître le rôle de l’échocardiographie dans l’évaluation et le suivi des patients
avec endocardite avérée ou suspectée.
➤Reconnaître une multitude de présentations échocardiographiques de l’endocardite
et de ses complications.

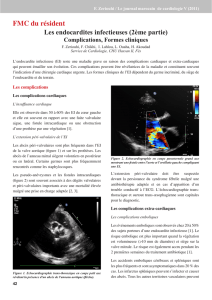
L’ENDOCARDITE INFECTIEUSE: SON PROFIL
➤Demeure un défi diagnostique et thérapeutique
➤Incidence stable
➤Évolution de son profil épidémiologique
➤Staph Aureus: Agent pathogène le plus communément identifié dans le monde
industrialisé
➤Modification des caractéristiques des patients:
➤Augmentation de l’âge moyen
➤Augmentation de la proportion des cas de valves prothétiques et de corps étrangers
intra-cardiaques
➤Diminution de la proportion des cas de maladie rhumastismale
Baddour, Larry M. Circulation. 2015;132:00-00
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
1
/
40
100%