Chimiothérapie néoadjuvante focus sur les tumeurs du sein triple

Chimiothérapie
néoadjuvante
néoadjuvante
focus sur les tumeurs
du sein triple négatives
Frédérique Penault-Llorca, MD, PhD
ERTICa
EA 4677 Université d
’
Auvergne
ERTICa
EA
4677
Université
dAuvergne
Centre Jean Perrin
Clermont-Ferrand
France

Incidence
/
mortalité
/
•1985 : 25.000 NC et 9 200 décès
•2002 : 42.000 NC (+ 35 % en 10 ans) et 11 000 décès
•
2012 : 55 000 NC et 11 500 décès
•
2012
:
55
000
NC
et
11
500
décès
•L'augmentation de incidence intéresse toutes les
tranches d'âge - Age moyen de survenue : 57 ans
–
50 % surviennent chez les plus de 70 ans
50
%
surviennent
chez
les
plus
de
70
ans
–Rare chez la femme avant 35 ans : 5 %

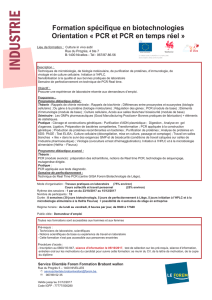
Ratio incidence/mortalité
Ratio
incidence/mortalité
•Incidence croissante augmentation du Nb de
li é bl
féi
=
morta
li
t
é
sta
bl
e
f
emmes gu
é
r
i
es
•Ratio incidence/mortalité en Europe
France 0,29
Pays-Bas 0,35
Danemark 0,39
Espagne 0,39
Italie
040
Italie
0
,
40
Royaume-Uni 0,43

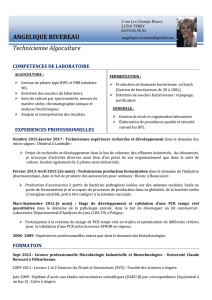
« cancer du sein et survie»
Données historiques
•
Middlesex
hospital
: données historiques
Middlesex
hospital
:
données
historiques
observationnelles sur 250 cancers du sein en situation
avancée (74% M, 23% stades III° traités entre 1805 et
1933:
–Survie médiane:
27
2
,
7
ans
–44% en vie à 3 ans
–18% à 5 ans
4% en vie à 10 ans
A 5 ans toutes les patientes porteuses de cancer de grade élevé
–
A
5
ans
toutes
les
patientes
porteuses
de
cancer
de
grade
élevé
ou III sont décédées
Bloom HJ. The natural history of untreated breast cancer. Ann N Y Acad Sci. 1964 ;114:747-54.

Mortalité
Mortalité
•
2012 : 11 500 décès (18% des décès alors que >1/3
2012
:
11
500
décès
(18%
des
décès
alors
que
>1/3
cancers)
di d fd
•Taux
d
e surv
i
e tous sta
d
es con
f
on
d
us :
74 % à 5 ans et 58% à 10 ans
•Stabilité, voire légère décroissance de la mortalité globale
•
Origine
:
Origine
:
–Dépistage (diminution du risque de décès par cancer du sein de
35%)
35%)
–Qualité du traitement loco-régional,
Dtit tdj t
–
D
es
t
ra
it
emen
t
s a
dj
uvan
t
s
–Et de la personnalisation des traitements
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
1
/
93
100%