Cœur pulmonaire chronique post

When heart failure has to do with
past abdominal surgery…
Julien PLESSIS
Journées Françaises de l’Insuffisance
cardiaque
Toulouse, vendredi 13 septembre 2013

Cas clinique
•Mme S, 70 ans, adressée par son pneumologue
pour bilan d’HTAP
•Antécédents :
–FA persistante
–Cholécystectomie ancienne
–Thyroïdectomie ancienne, hypothyroïdie
supplémentée
–Obésité morbide (IMC à 45 kg/m²)
•TTT : Euthyral, Coumadine, Avlocardyl 160 mg 2/j,
Lasilix 40 mg/j, Aldactone 25 mg/j

•Bilan pulmonaire :
–ETT : FEVG conservée, cavités droites dilatées +++, PAPS à
60 mmHg (IT)
–Test de marche 6 min : distance parcourue 255 m (94% de la
théorique), pas de désaturation
–Scintigraphie pulmonaire V/P: Absence de troubles
perfusionnels
–EFR : Syndrome restrictif par obésité, VEMS à 66%, CPT à
68 %
–GDS : PaCO2 43,5 mm Hg, PO2 82,5 mm Hg
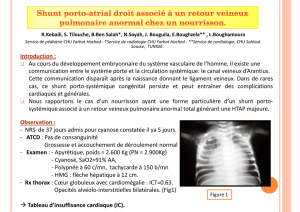
–TDM thoracique : cardiomégalie, dilatation des artères
pulmonaires

•A son admission :
– Signes d’insuffisance cardiaque globale
–Poids 137 kg pour 159 cm (IMC à 54 kg/m²)
•ECG : FA à 110 bpm, QRS fins
•Biologie :
–Créatininémie 87 µmol/l,
–Bilan hépatique : pas de cytolyse, cholestase
minime (2N), bilirubine totale 27 µmol/l
–Hb : 13,2 g/dl

•Cathétérisme droit :
–Volémie très imparfaitement contrôlée (POD à
20 mm Hg)
Traitement déplétif
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
1
/
25
100%