Langerhans Cell Histiocytosis Mimicking Periapical Pathology
Telechargé par
Maroua Bouflija

Langerhans Cell Histiocytosis Mimicking
Periapical Pathology in a 39-Year-Old Man
Scott M. Peters, DDS,*Julie Pastagia, DMD,
†
Angela J. Yoon, DDS, MAMSc, MPH,*
and Elizabeth M. Philipone, DMD*
Abstract
Langerhans cell histiocytosis (LCH) is a clonal neoplastic
proliferation of Langerhans-type dendritic cells, with
more than 50% of cases of LCH seen in children younger
than 15 years of age. The most common clinical presen-
tation of LCH is solitary or multiple bony lesions. The
jaws are affected in approximately 10%–20% of cases,
with a strong predilection for the mandible. The maxilla
is involved in only 1% of head and neck cases. When the
jaws are involved, lesions of LCH may mimic periapical
pathology as seen in patients requiring endodontic ther-
apy or bone loss as seen in periodontal disease. We
report the case of a 39-year-old man with LCH involving
the posterior maxilla. This is a rare presentation of LCH
with respect to both location and patient age. Clinicians
should consider LCH when developing a differential
diagnosis of an apical radiolucency of vital teeth or teeth
that fail to respond to endodontic therapy and be aware
of its clinical and radiographic mimics.
(J Endod 2017;-
:1–6)
Key Words
Langerhans cell histiocytosis, periapical pathology,
posterior maxilla
Langerhans cells are
dendritic cells of the
skin and mucosa from
which 2 main subgroups
of tumors can arise. The
first, Langerhans cell his-
tiocytosis (LCH), refers to
a clonal neoplastic prolif-
eration of Langerhans-
type cells, whereas the second, Langerhans cell sarcoma, is a high-grade neoplasm
with overtly malignant cytologic features (1).
LCH was classically referred to as histiocytosis X; this condition was further sub-
divided into 3 categories depending on the clinical presentation (2). Eosinophilic gran-
uloma was the term used for a solitary or multiple bony lesions without visceral
involvement. If multiple lesions involving the bone, skin, and viscera were present,
the condition was referred to as Hand-Sch€
uller-Christian disease. Prominent cutaneous,
bone marrow, and visceral involvement occurring mainly in infants was termed
Letterer-Siwe disease. These classical designations were often unclear because of over-
lapping clinical features, and the generic term of Langerhans cell histiocytosis was later
introduced (3, 4).
In the current classification system, LCH is categorized on the basis of degree of
organ involvement. According to this system, lesions are first designated as having single
organ involvement or multiorgan involvement. Those affecting only a single organ, typi-
cally the bone or skin, are further classified as unifocal or multifocal. On the other hand,
multiorgan involvement is further categorized by the presence or absence of organ
dysfunction. If organ dysfunction is present, the condition is considered to be high
or low risk on the basis of which organs are involved (high risk includes lung, liver,
spleen, and/or bone marrow, and low risk includes skin, bone, lymph nodes, and/
or pituitary gland) (5–8).
LCH is a rare disease with an incidence of 5 cases per 1 million per year (9). More
than 50% of cases are seen in children younger than 15 years of age. LCH has a definite
male predilection, with a male to female ratio of 3.7:1 (10). The clinical presentation of
LCH varies, but in more than half of cases (55%) the disease is limited to one organ
(10). The bone is affected most frequently, followed by skin, lymph nodes, liver, spleen,
oral mucosa, lung, and central nervous system (6). Most commonly, bony lesions occur
in the skull, ribs, vertebrae, and mandible (11). In addition, there appears to be a cor-
relation between age of onset of LCH and the bones that are affected by the disease. Chil-
dren younger than 10 tend to have skull and femoral lesions (9), whereas those older
than 20 are more likely to have rib, shoulder girdle, and mandibular lesions (12). Other
clinical presentations depend on the organs involved by the disease process and can
include lymphadenopathy, diabetes insipidus, hepatosplenomegaly, and cytopenia
(13).
Bone lesions, either solitary or multiple, are the most common clinical presenta-
tion of LCH (14). Radiographically, the lesions appear as punched out radiolucencies
without cortication. The jaws are affected in 10%–20% of all cases (15). The most
frequently affected intraoral site is the posterior mandible, and here lesions may appear
scooped out or scalloped as a result of the destruction of superficial alveolar bone (16).
With advanced bone destruction, clinical symptoms may mimic those of severe chronic
From the *Division of Oral and Maxillofacial Pathology,
Columbia University College of Dental Medicine, New York;
and
†
Periodontist, Private practice, Manhattan, New York
Address requests for reprints to Dr Elizabeth M. Philipone,
Columbia University Medical Center, 630 West 168th Street,
PH15W-1562, New York, NY 10032. E-mail address:
0099-2399/$ - see front matter
Copyright ª2017 American Association of Endodontists.
http://dx.doi.org/10.1016/j.joen.2017.05.020
Significance
This is a rare presentation of Langerhanscell histio-
cytosis with regard to both its location (posterior
maxilla) and age of onset. Awareness of such pre-
sentation and consideration of Langerhans cell his-
tiocytosis in the differential diagnosis are critical in
patient management.
Case Report/Clinical Techniques
JOE —Volume -, Number -,-2017 Langerhans Cell Histiocytosis of Maxilla 1

periodontitis, and the teeth are described as ‘‘floating in air’’ after the
loss of alveolar bone (16, 17). Patients may complain of dull pain or
tenderness as a result of intraosseous oral lesions. Patients may also
develop proliferative or ulcerative mucosal or gingival lesions if the
disease process spreads from the bone to adjacent oral soft tissues
(18, 19). Soft tissue lesions are also associated with pain, bleeding,
gingival inflammation, impaired healing, and halitosis (20).LCH has
a strong predilection for the mandible; maxillary involvement by LCH
is uncommon and occurs in only 1% of head and neck cases (5).
Here we report the case of a 39-year-old man with LCH involving
the posterior maxillary bone. The lesion presented as a periapical radio-
lucency associated with tooth #3, leading to initial improper manage-
ment with root canal therapy (RCT).
Case Presentation
A 39-year-old man presented to his periodontist with a chief
complaint of pain and swelling associated with tooth #3 (maxillary right
first molar). The patient reported that he had previously experienced
similar symptoms at that site 2 years ago. At that time he was seen by
an endodontist who prescribed antibiotics that were ineffective at alle-
viating the pain or swelling. A periapical radiograph was taken that
showed a possible area of decreased bone density around the distal
root of tooth #3, which may have been interpreted as periapical pathol-
ogy (Fig. 1). The tooth tested vital with both Endo Ice (Colt
ene/Whale-
dent Inc, Cuyahoga Falls, OH) and electric pulp testing; however, it was
subsequently treated endodontically via RCT.
The patient’s medical history is significant for an isolated lesion of
LCH diagnosed within the skull approximately 1 year ago. With regard to
the patient’s history of LCH, he first presented to his neurologist with
complaints of headaches refractory to nonsteroidal anti-inflammatory
drugs. A magnetic resonance imaging scan was performed that showed
a radiolucent lesion within the skull (Fig. 2). On the basis of the patient’s
symptoms and radiographic presentation, a presumptive clinical diag-
nosis of a meningioma was made. The lesion was then excised and sent
for pathologic analysis, at which time a final diagnosis of LCH was
rendered. No other lesions of LCH were observed on imaging at this
time.
On presentation to his periodontist, the patient was not in acute
distress. Clinical examination revealed a gingival swelling in the area
of tooth #3. A radiograph was taken that showed a radiolucency at
the apex of the RCT-treated tooth (Fig. 3). Different treatment
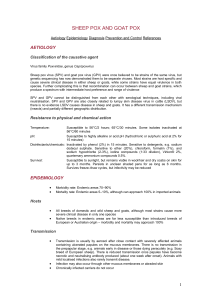
Figure 1. Pretreatment radiograph of tooth #3. Possible area of decreased
bone density, which may have been interpreted as periapical pathology, is pre-
sent around the distal root. Tooth tested vital with both electric pulp testing and
Endo Ice; however, RCT was performed. Triangular-shaped radiolucency ex-
tending from center of crown to coronal portion of root is a radiographic
artifact.
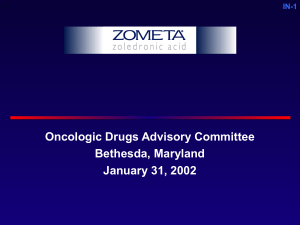
Figure 2. Sagittal (A) and coronal (B) magnetic resonance imaging scans showing lytic lesion at right skull base. Lesion is indicated with an asterisk (*).
Case Report/Clinical Techniques
2Peters et al. JOE —Volume -, Number -,-2017

options, including endodontic re-treatment and extraction, were dis-
cussed with the patient. The patient elected to have the tooth ex-
tracted.
The periodontist subsequently extracted tooth #3 and curetted out
the apical lesion and surrounding bone, which were sent for pathologic
analysis. The excised specimen consisted of 3 pieces of tissue ranging
from 0.1 to 0.5 cm in greatest dimension. Microscopic examination
showed pieces of edematous fibrous connective tissue infiltrated by
both acute and chronic inflammatory cells (Fig. 4A). Abundant eosin-
ophils were present, as well as atypical histiocytes with indented (kidney
bean shaped) nuclei (Fig. 4B). Also identified within the specimen were
small and thin-walled blood vessels and pieces of non-vital bone exhib-
iting loss of osteocytes from lacunae (sequestrum formation) and pe-
ripheral resorption (Fig. 4C).
Immunohistochemical analysis of the lesional tissue was per-
formed. The lesion was strongly positive for CD1a (Fig. 4D). Staining
results with S100, CD45, and langerin were also positive. CD138 stain
was negative. The Ki-67 proliferation index was moderately elevated.
Staining for BRAF was equivocal.
On the basis of the histologic findings, a diagnosis of LCH was
made. Because this was the second lesion of LCH in this patient, it
was recommended that he receive further testing to identify any addi-
tional lesions that may be present. The patient subsequently underwent
positron emission tomography/computed tomography imaging at Me-
morial Sloan Kettering Hospital, which showed no further evidence of
LCH but did reveal residual lesion in the area of tooth #3 that had
not been fully removed. The patient is currently under observation
Figure 3. Periapical radiograph of tooth #3 showing punched out radiolu-
cency at root apex. Tooth had been endodontically treated approximately
2 years before this radiograph was taken.
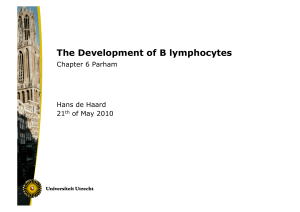
Figure 4. (A) Low-power image showing pieces of edematous fibrous connective tissue infiltrated by acute and chronic inflammatory cells (hematoxylin-eosin;
original magnification, 20). (B) On higher magnification, abundant eosinophils and atypical histiocytes with indented (kidney bean shaped) nuclei can be appre-
ciated (hematoxylin-eosin; original magnification, 400). (C) Also identified within the specimen are small and thin-walled blood vessels and pieces of non-vital
bone exhibiting loss of osteocytes from lacunae (sequestrum formation) and peripheral resorption. Abundant eosinophils are present ( hematoxylin-eosin; original
magnification, 200). (D) LCH, diffusely positive for CD1a (hematoxylin-eosin; original magnification, 20).
Case Report/Clinical Techniques
JOE —Volume -, Number -,-2017 Langerhans Cell Histiocytosis of Maxilla 3

TABLE 1. Reported Cases of Maxillary LCH
Author/year (reference) Case no.
Patient age
(y)/gender
Location of maxillary
involvement Additional lesions Treatment
Years of follow-up/
outcome
Schepman et al/1998
(31)
1 3/m Posterior, multifocal Mandible Surgery None provided
2 19/m Posterior, multifocal Mandible Chemotherapy 1.5/extension of oral
lesions
3 23/m Anterior and posterior Mandible and extraoral Surgery, radiotherapy,
and chemotherapy
5/new oral lesions and
progression of
extraoral lesions
4 46/m Posterior, multifocal Mandible and extraoral Surgery and
chemotherapy
5/new oral lesions
Shao et al/2004 (32) 5 — — None Surgery None provided
6 — — Mandible Surgery None provided
7 — — Mandible Surgery None provided
Shekhar and
Ponnudurai/2009 (29)
8 4/m Right posterior Mandible Bone curettage 5.7/no new lesions
Jindal et al/2009 (28) 9 6/m Multifocal, anterior and
posterior
Mandible and skull Not discussed None provided
Abdul-Jalil and Hin-Lau/
2009 (30)
10 2/m Right posterior Mandible Not discussed None provided
11 1/f Left maxilla None Not discussed None provided
12 2/m Right alveolus and
palatal swelling
Skin rashes, scalp
lesions, orbital lesions
Not discussed None provided
13 2/f Multifocal Mandible Not discussed None provided
Azreen et al/2012 (33) 14 2/m Right maxillary sinus Orbit, skull, liver Chemotherapy 1/no new lesions
Terada/2013 (27) 15 46/m Not specified Mandible Bone curettage 2/no new lesions*
Vargas et al/2016 (20) 16 16/m Radiolucency apical to
tooth #14
None Lesion healed
spontaneously after
incisional biopsy
5/no new lesions
Peters et al/2017
(current case)
17 39/m Radiolucency apical to
tooth #3
Skull Extraction of tooth #3
and bone curettage
6 mo/no new lesions at
the time of writing
f, female; m, male.
*Patient has total follow-up time of 7 years. Maxillary lesion in this case occurred 5 years after initial diagnosis of mandibular lesion.
Case Report/Clinical Techniques
4Peters et al. JOE —Volume -, Number -,-2017

only at this time, with a plan to follow up every 3 months for reassess-
ment. At the time of writing, the patient has been followed for 6 months
without any new lesions.
Discussion
This case is an unusual presentation of LCH occurring as a peri-
apical radiolucency of the maxilla in an adult male. The jaws are affected
in 10%–20% of cases, with a strong predilection for the mandible (15).
Clinical and radiographic differential diagnosis often includes general-
ized chronic periodontitis, periapical granuloma, or periapical cyst.
Although these conditions will successfully respond to conventional
periodontal or endodontic therapy, oral manifestations of LCH will be
refractory to treatment, as was seen in our case. Histopathologic anal-
ysis is necessary to confirm a diagnosis of LCH. On hematoxylin-eosin
stain, Langerhans cells appear as large cells with grooved, folded, or in-
dented nuclei and an abundant eosinophilic cytoplasm. Nucleoli are not
well-appreciated in these cells (1, 11). Langerhans cells are often seen
in a mixed inflammatory background consisting of variable amounts of
neutrophils, eosinophils, histiocytes, and lymphocytes. Areas of
necrosis and hemorrhage may also be present (1, 10). Classically,
lesional Langerhans cells were identified by the presence of Birbeck
granules on electron microscopy (21). With the advent of immunohis-
tochemistry, diagnosis of LCH is now made after positive staining of le-
sional cells for CD1a and langerin. Lesional Langerhans cells will also
stain positive for S100, CD68, vimentin, HLA-DR, CD45, CD4, and lyso-
zyme. Other T-cell and B-cell markers, as well as follicular dendritic cell
markers, should not stain Langerhans cells (1, 10, 21).
The prognosis of LCH depends on the clinical stage at presentation.
Usually the prognosis is favorable when the disease is limited to a single
organ, with a survival rate of greater than 99%, but is less favorable with
multiorgan involvement, with a survival rate of approximately 33%
(10). Certain affected sites, such as the lung, liver, and bone marrow,
are associated with a worse prognosis (1). When LCH presents with
bony lesions, the treatment varies on the basis of the affected site. Easily
accessible locations, such as the mandible or maxilla, are treated with
curettage or intralesional injection of corticosteroid agents (22). Less
surgically accessible bony lesions are treated with radiation therapy.
Both single and multi-agent chemotherapy have also been used to treat
disseminated LCH, with low-dose cytosine arabinoside showing the best
response in adult patients (23, 24). In 40%–60% of LCH cases,
mutations in BRAF have been identified; however, the clinical and
prognostic implications of this mutation are unclear (25, 26).
Because of the rarity of LCH, it has been difficult to establish a gold
standard of treatment.
Although lesions of the skull and mandible are more frequently
seen in cases of LCH presenting in the head and neck, maxillary man-
ifestations of LCH are quite rare. Hicks and Flaitz (5) report that the
maxilla is involved in only 1% of head and neck cases. Within the pub-
lished literature, there are only a few documented cases of LCH occur-
ring within the maxillary bone. Vargas et al (20) describe a case of a
16-year-old male patient with an asymptomatic osteolytic lesion in
the periapical region of tooth #14 (left maxillary first molar). The lesion
was diagnosed as ‘‘monostotic eosinophilic granuloma of the maxillary
bone’’ on incisional biopsy. Surgical excision was planned as definitive
treatment; however, it was not performed because the lesion healed
spontaneously after the initial biopsy. Terada (27) reports a case of
recurrent multifocal LCH in a 46-year-old man. In this patient, osteolytic
lesions were found in both the mandible (3.0 1.0 1.0 cm) and the
maxilla (0.5 0.5 0.4 cm). Similarly, Jindal et al (28) and Shekhar
and Ponnudurai (29) document cases of oral LCH involving both the
mandible and maxilla. In a retrospective study by Abdul-Jalil and
Hin-Lau (30), the clinicopathologic presentation of oral LCH in Malay-
sian children was examined during a 40-year time period. Of the 17
cases of LCH documented, only 2 occurred solely in the maxilla, and
an additional 2 involved both the maxilla and mandible. Schepman
et al (31) provided a retrospective report of 11 cases of LCH affecting
the jaw bones. They reported maxillary involvement in 4 of these cases,
each with concurrent mandibular lesions. Shao et al (32) analyzed 21
cases of LCH with jaw involvement and found that only 1 of these cases
solely affected the maxilla, and an additional 2 involved both the maxilla
and the mandible. Azreen et al (33) reported a case of a 2-year-old boy
with multiorgan LCH involving the maxillary sinus. In this case, however,
no osteolytic lesion of the bone proper was observed. A complete listing
of the reported cases of maxillary LCH can be found in Table 1.
Our case adds an additional report of oral LCH, but in the uncom-
mon location of the posterior maxilla. Although maxillary involvement
by LCH has been described in the literature, the frequency of such
involvement is quite low, and most cases report osteolytic lesions in
both the maxilla and mandible. However, in our case, the mandible
was completely spared, although the patient did have a separate osteo-
lytic lesion of his skull. In addition, most documented cases of oral LCH
are seen in younger children; however, our patient is a 39-year-old
man.
In conclusion, one should consider the possibility of LCH when
developing a differential diagnosis for a radiolucent lesion of the maxilla
or mandible and be cognizant of its potential clinical and radiographic
similarities to more common periapical pathoses. Furthermore, when
weighing the likelihood of different diagnoses, one should not rule
out LCH simply on the basis of patient age, but rather a full work-up
of oral symptoms and evaluation of the patient’s medical history are
indicated to arrive at a diagnosis.
Acknowledgments
The authors deny any conflicts of interest related to this study.
References
1. Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Hae-
matopoeitic and Lymphoid Tissues, 4th ed. Lyon: International Agency for
Research on Cancer; 2008.
2. DiCaprio MR, Roberts TT. Diagnosis and management of Langerhans cell histiocy-
tosis. J Am Acad Orthop Surg 2014;22:643–52.
3. Abla O, Egeler RM, Weitzman S. Langerhans cell histiocytosis: current concepts and
treatments. Cancer Treat Rev 2010;36:354–9.
4. Lichtenstein L. Histiocytosis X: integration of eosinophilic granuloma of bone,
Letterer-Siwe disease, and Sch€
uller-Christian disease as related manifestations of
a single nosologic entity. AMA Arch Pathol 1953;56:84–102.
5. Hicks J, Flaitz CM. Langerhans cell histiocytosis: current insights in a molecular age
with emphasis on clinical oral and maxillofacial pathology practice. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 2005;100:42–66.
6. Satter EK, High WA. Langerhans cell histiocytosis: a review of the current recommen-
dations of the Histiocyte Society. Pediatr Dematol 2008;25:291–5.
7. Donadieu J, Chalard F, Jeziorski E. Medical management of Langerhans cell histio-
cytosis from diagnosis to treatment. Expert Opin Pharmacother 2012;13:1309–22.
8. Favara BE, Feller AC, Pauli M, et al. Contemporary classification of histiocytic
disorders: the WHO Committee on histiocytic/reticulum cell proliferations—
reclassification working group of the histiocyte society. Med Pediatr Oncol
1997;29:157–66.
9. Nicholson HS, Egeler RM, Nesbit ME. The epidemiology of Langerhans cell histio-
cytosis. Hematol Oncol Clin North Am 1998;12:379–84.
10. Aster JC, Pozdnyakova O, Kutok JL. Hematopathology. Philadelphia: Elsevier; 2013.
11. Ardekian L, Peled M, Rosen D, et al. Clinical and radiographic features of eosino-
philic granuloma in the jaws: review of 41 lesions treated by surgery and low grade
radiotherapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:238–42.
12. Miyamoto H, Dance G, Wilson DF, et al. Eosinophilic granuloma of the mandibular
condyle. J Oral Maxillofac Surg 2000;58:560–2.
13. Campos MK, Viana MB, de Oliveria BM, et al. Langerhans cell histiocytosis: a 16 year
experience. J Pediatr (Rio J) 2007;83:79–86.
Case Report/Clinical Techniques
JOE —Volume -, Number -,-2017 Langerhans Cell Histiocytosis of Maxilla 5
 6
6
1
/
6
100%