Phase III Trial

Cancer du pancréas : Référentiel et nouveautés
J.L. VAN LAETHEM,MD,PhD
Unité d’oncologie digestive
Erasme University Hospital
ULB-Brussels

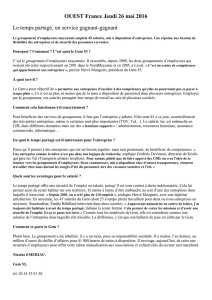
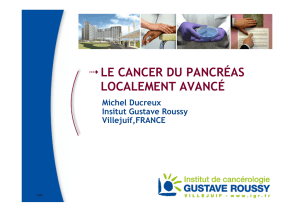
Late diagnosis
Palliative treatment
90% R0 surgery
10%
Metastatic LAD
disease
3-6 months 8-12 months
5 y. survival: 10-20%
18-20 months
MEDIAN SURVIVAL
PANCREATIC CANCER

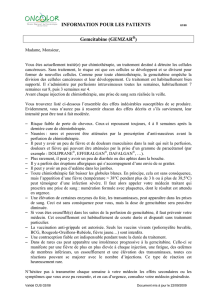
Ere du 5FU et des « BSC »
Ere de la Gemcitabine
Ere des cytotoxiques combinés
Ere des agents biologiques
Chemo(bio)radiation
Options thérapeutiques
dans le cancer du pancréas
1.Approche systémique <> métastatique
2.Approche Loco-régionale
3.Approche curative

INNOVONS !!!
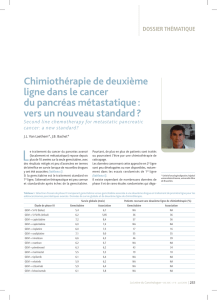
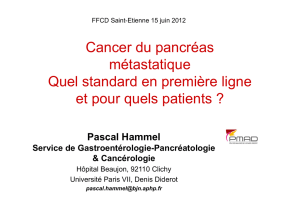
1997 : the Burris study Gemcitabine as a new
standard : median survival =6 months
1997-2006 : no major benefit of combining
cytotoxics,no new active chemotherapy
2005-2007 : anti EGFR therapy erlotinib added to
GEM : small benefit in survival (+ 0.5 month !) ; better
in patients with grade 2 rash
2007: biologics disappointing ! No survival benefit
median survival = 6.4 months

Traitement systémique
Quel standard?
Quels cytotoxiques?
Apport des biologiques?
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
1
/
64
100%