Trends in Cancer Incidence in Maputo, Mozambique, 1991–2008

RESEARCH ARTICLE
Trends in Cancer Incidence in Maputo,
Mozambique, 1991–2008
Cesaltina Lorenzoni
1,2
, Alba Vilajeliu
3,4
, Carla Carrilho
1,2
, Mamudo R. Ismail
1,2
,
Paola Castillo
3
, Orvalho Augusto
5
, Alberto L. García-Basteiro
3,7
, Mohsin Sidat
5
, Silvia de
Sanjosé
6
, Clara Menéndez
3,7
, Jaume Ordi
3,8
*
1Department of Pathology, Maputo Central Hospital, Maputo, Mozambique, 2Faculty of Medicine, Eduardo
Mondlane University, Maputo, Mozambique, 3ISGlobal, Barcelona Ctr. Int. Health Res. (CRESIB), Hospital
Clínic—Universitat de Barcelona, Barcelona, Spain, 4Department of Preventive Medicine and
Epidemiology, Hospital Clinic, Universitat de Barcelona, Barcelona, Spain, 5Department of Microbiology,
Faculty of Medicine, Eduardo Mondlane University, Maputo, Mozambique, 6Unit of Infections and Cancer,
Institut Catala d'Oncologia, L'Hospitalet de Llobregat, Barcelona, Spain, 7Centro de Investigação em Saúde
de Manhiça (CISM), Maputo, Mozambique, 8Department of Pathology, Hospital Clinic, Universitat de
Barcelona, Barcelona, Spain
Abstract
Background
Very limited information is available regarding the incidence of cancer in sub-Saharan
Africa. We analyzed changes in cancer patterns from 1991 to 2008 in Maputo
(Mozambique).
Methods
We calculated the rates of incidence of different cancer sites by sex in the 5-year age-group
of the population of Maputo city as well as age-standardized rates (ASRs) and average
annual percentage changes (AAPC).
Results
Over the 18-year study period a total of 12,674 cases of cancer (56.9% females) were regis-
tered with an overall increase in the risk of cancer in both sexes. In males, the most common
cancers were those of the prostate, Kaposi sarcoma (KS) and the liver. Prostate cancer
showed the most dramatic increase over the whole study period (AAPC +11.3%; 95% CI:
9.7–13.0), with an ASR of 61.7 per 10
5
in 2003–2008. In females, the most frequent cancers
were of the uterine cervix, the breast and KS, with the former increasing along the whole
study period (AAPC + 4.7%; 95% CI: 3.4–6) with an ASR of 62.0 per 10
5
in 2003–2008 as
well as breast cancer (AAPC +6.5%; 95%CI: 4.3–8.7).
Conclusions
Overall, the risk of cancer rose in both sexes during the study period, particularly among
cancers associated with westernization of lifestyles (prostate, breast), combined with
PLOS ONE | DOI:10.1371/journal.pone.0130469 June 25, 2015 1/12
OPEN ACCESS
Citation: Lorenzoni C, Vilajeliu A, Carrilho C, Ismail
MR, Castillo P, Augusto O, et al. (2015) Trends in
Cancer Incidence in Maputo, Mozambique, 1991–
2008. PLoS ONE 10(6): e0130469. doi:10.1371/
journal.pone.0130469
Academic Editor: Aamir Ahmad, Wayne State
University School of Medicine, UNITED STATES
Received: January 5, 2015
Accepted: May 20, 2015
Published: June 25, 2015
Copyright: © 2015 Lorenzoni et al. This is an open
access article distributed under the terms of the
Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any
medium, provided the original author and source are
credited.
Data Availability Statement: All relevant data are
within the paper.
Funding: The authors have no support or funding to
report.
Competing Interests: The authors have declared
that no competing interests exist.

increasingly rising incidences or limited changes in cancers associated with infection and
poverty (uterine cervix, liver). Moreover, the burden of AIDS-associated cancers has shown
a marked increase.
Introduction
Knowledge of cancer patterns in the different populations is crucial to guide preventive efforts
[1–4]. For this reason, cancer registries have been developed to record epidemiological data
that are used to guide cancer prevention and control programs [1–5]. Unfortunately, very lim-
ited information is available regarding the incidence of cancer in sub-Saharan Africa[1,4–6].
This may be due to different reasons including limited resources in collecting and registering
information as well as the lack of stability in maintaining registries over long periods of time.
All of this has precluded evidence-based analysis of time patterns related to the incidence of
cancer in this region[4,7,8].
After the end of the civil war in 1991 the Department of Pathology of the Maputo Central
Hospital (MCH) started a cancer registry with the aim of obtaining information on the occur-
rence of cancer in the population of Maputo city. This lengthy registration of data has provided
a unique opportunity to study temporal trends in cancer patterns in an African setting.
Interestingly, epidemiological data had previously been obtained by the Department of
Pathology of the MCH (then known as Miguel Bombarda Hospital) from 1956 to 1961 in a
cancer survey covering the metropolitan area of 60 square kilometers of Maputo (then known
as Lourenço Marques) [9].
More than 50 years later, significant social and epidemiological changes have taken place in
Mozambique, with a progressive urbanization of the population and the eruption of the HIV
epidemic which has disproportionately affected many sub-Saharan African countries[9].
In the present study we analyzed the changes in cancer patterns in Maputo city, Mozam-
bique from 1991 to 2008.
Materials and Methods
Study Site
This study was performed in the Department of Pathology of the MCH, a 1500-bed hospital
that is the only quaternary care center in Mozambique and is a national referral center. This
department primarily serves the Southern Zone of Mozambique including Maputo and its sur-
roundings (provinces of Maputo, Gaza and Inhambane), with a small proportion of cases
derived from other areas of the country due to the national referral nature of the institution.
The department receives virtually all specimens from the city of Maputo. The department has a
database of all the samples received for pathological diagnosis including specimens of most
types of cancers (with the exception of leukemia and cancers with only a clinical diagnosis).
Study Design
This study was approved by the National Bioethics Committee of Mozambique, and the
Mozambican Ministry of Health (Ref. 389/CNBS). The analysis included all the cases of cancer
registered in the Department of Pathology of the MCH from January 1, 1991 to December 31,
2008. Data were entered into a Microsoft Access database (Microsoft Co, Redmond, WA,
USA) which, upon data entry, prevents the use of nonexistent codes and performs checks for
Trends in Cancer Incidence in Mozambique
PLOS ONE | DOI:10.1371/journal.pone.0130469 June 25, 2015 2/12

internal consistency between variables. The database was carefully reviewed (name, age) to
confirm that no duplications had been registered. Information about previous analyses in the
same patient was also obtained, in order to identify potential duplicate registrations. Cases
were identified in the registries as histological studies (including biopsies and surgical pathol-
ogy), cytological specimens, and autopsies. For each case identified basic demographic data
were collected, including age, sex and address. Patients from sites other than Maputo were
excluded. For each specimen, the date of diagnosis, method of diagnosis, site from which the
specimen was taken (topography), and microscopic morphology were recorded. Patient rec-
ords/information were anonymized and de-identified prior to analysis. All topographic and
morphologic classifications were made according to the International Classification of Diseases
for Oncology (ICD-O)[10,11] and were converted into the 10
th
version of the ICD[12]. In con-
cordance with other cancer registries, cancers such as Kaposi’s sarcoma and malignant lym-
phomas were not classified by localization, as they are considered multifocal, and were
included only once in the analysis[5,7]. Multiple cancers occurring in the same patient were
entered as separate cases. Squamous cell carcinomas (SCCs) of the conjunctiva were defined as
tumors with ICD-O morphology codes M8010–M8082 of conjunctiva ICD-O C69.0) or eye,
unspecified (ICD-O C69.9).
Population
Censuses of the population of Mozambique were performed in 1980[13], 1997[14] and 2007
[15], providing demographic information of Maputo by sex and 1 year of age groups for these
years. Intercensal estimates were calculated assuming a constant rate of change in growth
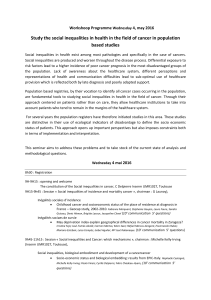
within sex and age groups. Fig 1 shows the population of Maputo by gender and age groups in
the censuses of 1997 and 2007.
Statistical Analysis
The rates of incidence of cancer were calculated for the 5-year age-group by sex, for each year
(1991–2008) and for three time periods: 1991–1996, 1997–2002 and 2003–2008. Age-standard-
ized rates (ASRs) were calculated using the world standard population[16]. The average annual
percentage change (AAPC) and 95% confidence intervals (95%CI) over the 18-year study
period were calculated for each sex and cancer sites. The AAPC was estimated on fitting a Pois-
son regression model to the natural logarithm of the counts offset for the logarithm of the per-
son-years, including the calendar period as a continuous variable to estimate the slope. The
calculation of the AAPC assumes that the rates increase or decrease log-linearly over the entire
period[17,18]. Graphs on time trend estimates show 3-year moving average values of rates to
minimize fluctuation due to small numbers of cases.
Results
During the 18 years of registration included in the analysis (1991–2008) a total of 12 674 cases
(5415 males and 7208 females, sex not recorded in 51) were registered. The rates of the inci-
dence of cancer were shown to have increased in both sexes over the study period with an
AAPC of +4.8% (95% CI: 4.0–5.5) for males and +5.1% (95% CI: 4.3–5.9) for females. The ASR
for the 1991–1996 period was 102.3 per 10
5
in males and 102.6 per 10
5
in females, being 182.7
per 10
5
in males and 186.0 per 10
5
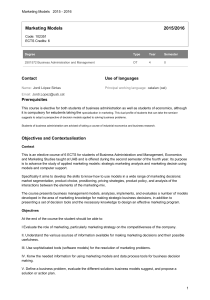
in females in the period from 2003–2008. Fig 2 shows the
age-specific incidence for all cancers in the three time periods by sex and the trends in inci-
dence of the four most frequent tumors in males and females. In males, the most common can-
cers along the study period (in terms of ASRs) were those of the prostate, Kaposi’s sarcoma
(KS), the liver and the esophagus (Table 1;Fig 2C). Prostate cancer showed the most dramatic
Trends in Cancer Incidence in Mozambique
PLOS ONE | DOI:10.1371/journal.pone.0130469 June 25, 2015 3/12


increase over the whole study period (AAPC +11.3%; 95% CI: 9.7–13.0), with an ASR of 61.7
per 10
5
in 2003–2008 (Table 1). During the study period the increase in the incidence of pros-
tate cancer was greater in subjects over 60 years of age compared to younger subjects (35.1 per
10
5
versus 3.9 per 10
5
)(Fig 3A). The age of patients with cancer of the liver varied widely, with
78.1% diagnosed in patients younger than 60 years of age (Fig 3B).
In females, the most frequent cancers over the whole study period were cancer of the uterine
cervix, breast, KS and the liver (Table 1;Fig 2D). Cancer of the uterine cervix increased along
the study period (AAPC + 4.7%; 95% CI: 3.4–6) with an ASR of 62.0 per 10
5
in 2003–2008
(Table 1). The increases in the incidence of both cancer of the uterine cervix and the breast
tended to be higher in women older than 40 years of age (41.9 per 10
5
versus 6.3 per 10
5
for
cancer of the uterine cervix and 16.3 per 10
5
versus 2.1 per 10
5
for breast cancer) (Fig 3C and
3D). The incidence of KS was shown to markedly increase along the study period in both gen-
der groups and in all age groups (Fig 3E and 3F).
Among children (0–14 years) 738 cancers were registered during the 18-year study period.
Of the 738 pediatric tumors 420 (56.9%) occurred in males, 311 (42.1%) in females and in 7
cases the sex was not recorded. The most common tumors were non-Hodgkin’s lymphomas
Fig 2. Age-specific incidence rates of male (A) and female (B) cancers in the periods 1991–1996, 1996–2001 and 2003–2008; and trends in age-
standardized incidence rates of the four most frequent cancers in males (C) and females (D) from 1991–2008.
doi:10.1371/journal.pone.0130469.g002
Trends in Cancer Incidence in Mozambique
PLOS ONE | DOI:10.1371/journal.pone.0130469 June 25, 2015 5/12
 6
7
8
9
10
11
12
6
7
8
9
10
11
12
1
/
12
100%