http://jid.oxfordjournals.org/content/198/2/218.full.pdf

Expression of Defective Hepatitis B Virus Particles
Derived from Singly Spliced RNA Is Related
to Liver Disease
Patrick Soussan,1,2,3,4,7 Jonathan Pol,1,2,3 Florianne Garreau,1,2,3 Veronique Schneider,4,7 Catherine Le Pendeven,4,7
Bertrand Nalpas,5,9 Karine Lacombe,4,10 Philippe Bonnard,8Stanislas Pol,1,5,6,9 and Dina Kremsdorf1,2,3
1Pathogenèse des Hépatites Virales B et Immunothérapie, Institut National de la Santé et de la Recherche Médicale (INSERM) U845,
2Département de Virologie, Institut Pasteur, 3Faculté de Médecine René Descartes, Université Paris 5, 4Université Pierre et Marie Curie, EA3500,
5Département d’Immunologie, Institut Cochin, and 6INSERM U567 and 7Laboratoire de Virologie and 8Services des Maladies Infectieuses et
Tropicales, Hôpital Tenon, 9Service d’Hépatologie, Hôpital Cochin, and 10Service de Maladie Infectieuse, Hôpital Saint Antoine, Assistance
Publique–Höpitaux de Paris, Paris, France
Background. Defective hepatitis B virus (HBV) particles, generated from singly spliced HBV RNA, have been
detected in chronic carriers of HBV. The present study was designed to quantify the expression of defective HBV
(dHBV) and wild-type HBV (wtHBV) genomes in the serum of patients with HBV infection and its relation to the
severity of liver disease.
Methods. HBV and dHBV loads were determined by quantitative polymerase chain reaction in the serum of 89
untreated HBV-infected patients (31 coinfected with human immunodeficiency virus [HIV] type 1) with liver disease
of different stages. The ratio of dHBV DNA to total (wtHBV plus dHBV) HBV DNA (dHBV/HBV ratio) was used to
express data independently of the level of viral replication.
Results. Despite a global correlation between dHBV and wtHBV load, the dHBV/HBV ratio ranged from 0.001%
to 69%. The variation in dHBV/HBV ratio was independent of HIV coinfection, HBV genotype, and precore muta-
tions. The mean dHBV/HBV ratio was higher in patients with severe liver necrosis and fibrosis.
Conclusions. Our data indicate that an elevated dHBV/HBV ratio is associated with liver necroinflammation and
fibrosis disease, suggesting a regulation of dHBV expression according to the severity of the liver disease. The dHBV/
HBV ratio may help to better define liver disease stage during HBV infection.
Persistent human hepatitis B virus (HBV) infection is a
major public health problem. The major complications
of chronic HBV infection are the development of liver
cirrhosis and hepatocellular carcinoma (HCC) [1–3].
Evidence indicating a direct involvement of HBV in this
process is now available [3]; indeed, recent data have
demonstrated that serum HBV DNA levels are strong
predictors of the risk of HCC, independent of hepatitis B
e antigen (HBeAg) expression, serum alanine amino-
transferase (ALT) level, and liver cirrhosis [4]. More-
over, retrospective studies have shown that HBV geno-
type and HBeAg expression may also increase the risk of
HCC [5, 6]. In addition, the effect of HBV genetic vari-
ability, including precore (preC) mutants and viral ge-
notype, has been implicated in liver disease progression
[7]. Furthermore, HIV-1 infection in HBV-infected pa-
tients increases the level of HBV DNA and the risk of
cirrhosis [8]. HBV should therefore be considered as
having synergistic effects with chronic inflammation in
the pathogenesis of liver disease.
HBV is a small, enveloped DNA virus and is a member
of the hepadnavirus family; its genome consists of a re-
laxed, circular, partially double-stranded 3.2-kb DNA
molecule [9]. Five unspliced messenger (mRNA) tran-
scripts of 3.5 (short and long), 2.4, 2.1, and 0.8 kb are
synthesized from the HBV genome and encode for the
capsid, envelope, polymerase, and transactivator X viral
proteins [9]. The 3.5-kb short pregenomic mRNA is also
involved in the HBV replication cycle via its reverse tran-
Received 31 August 2007; accepted 12 February 2008; electronically published
4 June 2008.
Potential conflicts of interest: none reported.
Financial support: Institut National de la Santé et de la Recherche Médicale;
Agence Nationale de Recherche sur le SIDA et les Hépatites Virales (grant
A020042 to the study); French Research Ministry (grant to J.P.).
Reprints or correspondence: Dr. Patrick Soussan, INSERM U845, CHU Necker,
156 rue de Vaugirard 75015, Paris, France ([email protected]).
The Journal of Infectious Diseases 2008; 198:218–25
© 2008 by the Infectious Diseases Society of America. All rights reserved.
0022-1899/2008/19802-0010$15.00
DOI: 10.1086/589623
MAJOR ARTICLE
218 ●JID 2008:198 (15 July) ●Soussan et al.

scription, which occurs in core particles [9]. In addition to un-
spliced HBV mRNA, singly and doubly spliced 2.2-kb mRNAs
arising from 3.5-kb pregenomic mRNA have been identified in
HBV DNA–transfected cell lines and in HBV-infected liver [10 –
16]. The major spliced HBV mRNA that lacks intron 2447/489
accounts for up to 30% of pregenomic transcripts, as revealed in
transfected cells and in the livers of chronically infected patients
[10 –13]. The mechanism for the regulation of splicing is still not
clearly understood. Unlike the retrovirus model, the influence of
HBV protein expression and viral genetic variability on splicing
regulation has never been investigated. However, a recent report
suggested that the posttranscriptional regulatory element, which
is involved in the nuclear export of intronless viral subgenomic
RNAs, presents regulatory elements that control viral prege-
nome processing by stimulating or inhibiting splicing [17]. We
and others have shown that spliced mRNA is packaged, reverse
transcribed, and leads to the secretion of defective viral particles
[14, 15, 18 –20]. Defective viruses are maintained in the popula-
tion through transcomplementation with wild-type helper virus
[18]. The regulation of spliced HBV RNA packaging is not well
defined; however, recent data have indicated that mutations
within the C-terminus of HBV core protein may influence the
encapsidation of spliced HBV RNA [21, 22]. In addition, the
processing of defective HBV (dHBV) secretion may differ from
that of wild-type HBV (wtHBV) secretion [20].
Defective HBV genomes contain open reading frames that
may encode for various fusion and truncated proteins. It has
been reported that a polymerase and surface fusion protein en-
coded by spliced RNA is incorporated into viral particles and
may then play a role in the viral life cycle [16]. In addition, it has
also been demonstrated that the expression of spliced duck HBV
RNA encoding for the large surface protein is important for rep-
lication in infected hepatocytes [23]. In woodchucks chronically
infected with woodchuck hepatitis virus (WHV), 2 different
spliced WHV RNAs potentially encoding for core and polymer-
ase fusion proteins were secreted as defective particles [24, 25].
The most frequently detected dHBV genomes result from the
reverse transcription of singly spliced 2.2-kb mRNAs [14]. We
previously demonstrated that this spliced HBV genome leads to
the in vivo expression of a new HBV splice– generated protein
(HBSP), which corresponds to fusion of the N-terminal part of
polymerase and a new open reading frame created by the single
splicing event [26]. HBSP expression did not modulate the level
of HBV replication, but indirect in vivo detection of HBSP may
be related to viral load and liver fibrosis [27].
Overall, it is clear that dHBV particles are present in the liver
and serum of chronically infected patients. However, the clinical
impact of their expression during liver disease remains to be
established. The aim of the present study was, therefore, to quan-
tify dHBV and wtHBV particles in serum samples and to evalu-
ate the impact of HBV genetic variability and liver status on
dHBV particle expression in untreated individuals with chronic
HBV infection.
METHODS
Patients and samples. Eighty-nine chronic HBV carriers who
were positive for hepatitis B surface antigen, had a detectable
HBV load, were negative for markers of hepatitis C and D virus,
and had never received anti-HBV therapy were randomly in-
cluded in our study (table 1). Untreated patients were selected to
avoid any bias resulting from HBV fitness due to antiviral treat-
ment. Of the selected patients, 31 were coinfected with HIV-1.
HIV coinfection is usually associated with rapid progression to
liver cirrhosis [8]. ALT activity and HBeAg levels were evaluated
by standard biological assays (bioMérieux). For HBV/HIV-
coinfected patients, CD4 cell count (Coulter) and HIV load
(Bayer) were quantified. Liver biopsy specimens were obtained
during a 3-month period around the date of serum sample, em-
Table 1. Clinicopathological data on patients with chronic hepatitis B virus (HBV) infection (nⴝ89).
Parameter HBV monoinfection HBV/HIV coinfection
Sex, no. male/female 43/15 29/2
Age, years 34 ⫾10 (19–81) 36 ⫾5 (22–50)
HIV load, copies/mL . . . 8.8 ⫻104⫾5.1 ⫻104(⬍500–323,500)
CD4 cell count, cells/mm3... 428⫾250 (45–856)
Alanine aminotransferase level, IU/L 107 ⫾15 (17–610) 74 ⫾14 (16–374)
METAVIR histological score, no. of patients
Liver necroinflammation
A0–A1 28 6
A2–A3 30 13
Liver fibrosis
F0–F2 27 21
F3–F4 31 10
NOTE. Data are means ⫾SEs (ranges), unless otherwise specified.
Defective HBV Particles and Liver Disease ●JID 2008:198 (15 July) ●219

bedded in paraffin, and sectioned; sections were stained with
hematoxylin-eosin. Liver biopsy specimens were classified as ex-
hibiting no or moderate (A0 –A1) or severe (A2–A3) liver necro-
sis and no or moderate (F0 –F2) or severe (F3–F4) liver fibrosis,
using the METAVIR scoring method. For 12 patients with
HIV-1 coinfection, the fibrosis score was evaluated by high-
resolution real-time ultrasound on the basis of a quantitative
scoring system. Necroinflammation scores were not available for
these 12 patients.
Real-time polymerase chain reaction (PCR). HBV DNA
was extracted from serum samples (200
L) by means of a spin
column (Qiagen) and eluted in 200
L of water. Real-time quanti-
tative PCR was performed using the LightCycler system (Roche) in
20
L of LightCycler DNA Master SYBR Green Mix (Roche) con-
taining 3 mmol/L MgCl2and 2
L of viral DNA extract. The dHBV
primers were 5'-AGTGTGGATTCGCACTCC-3' (forward; nt
2271–2289) and 5'-CTGGTTGTTGATGATCATT-3' (reverse; nt
504 – 489^2447–2445); the wtHBV primers, forward 5'-ATCTT-
CTTGTTGGTTCTTCT-3' (forward; nt 430 – 450) and 5'-CTGA-
AAGCCAAACAGTGG-3' (reverse; nt 733–715). Each PCR cycle
comprised denaturation at 95°C for 20 s, annealing at 65°C for
15 s, and extension at 72°C for 12 s (45 cycles). The standard
curve for quantification was calculated using serial 10-fold (500
to 1011 copies/mL) dilutions of wtHBV or dHBV plasmids.
Analysis of HBV genotypes and preC mutants. To detect
mutations in the HBV basal core promoter (BCP) and preC regions
and to determine HBV genotypes, a 644-bp fragment including the
entire BCP (nt 1742–1849) and preC (nt 1814 –1900) regions was
amplified using the primers 5'-CATGGACCACCGTGAAC-3'
(forward; nt 1605–1621) and 5'-AGTGCGAATCCACACTC-3'
(reverse; nt 2284 –2268) and was sequenced in an Applied Biosys-
tems 3100 automatic sequencer. In the BCP region, mutations in nt
1762–1764 were analyzed; in the preC region, all nucleotide changes
were analyzed. Viral genotypes were established by aligning the
preC/core (preC/C) sequences obtained with consensus sequences
of HBV genotypes A, B, C, D, E, F, and G from GenBank.
Statistical analysis. Statistical analysis was performed using
the nonparametric Mann-Whitney Utest; results are given as
means ⫾SEs and medians. The correlation assay was evaluated by
the Spearman rank correlation test (version 5.0; StatView software)
(SAS). Analysis of variance was performed to compare HBV geno-
type. Differences were considered significant at P⬍.05. The Bon-
ferroni correction was used to determine the Pvalue cutoff for
liver status (ALT activity, liver necroinflammation, and fibrosis).
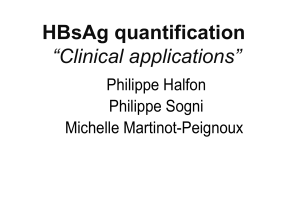
Figure 1. A, Schematic representation of wild-type hepatitis B virus (wtHBV) DNA and defective HBV (dHBV) DNA generated from singly spliced
2.2-kb HBV pregenomic RNA. For wtHBV, the gene encoding for polymerase is shown in light gray; for dHBV, the HBV splice–generated protein (HBSP)
gene, in frame with polymerase, is shown in light gray, whereas the 3' part encoding for the original sequence is shown in dark gray. Arrows indicate
the location of primers for specific amplification of either wtHBV or dHBV DNA. B, wtHBV and dHBV loads in patient groups 1 (HBV monoinfection) and
2 (HBV/HIV coinfection). Values for wtHBV and dHBV loads were determined by real-time quantitative polymerase chain reaction and are represented
using logarithmic scales.
220 ●JID 2008:198 (15 July) ●Soussan et al.

RESULTS
Quantification of dHBV and wtHBV DNA in the serum of
chronic HBV carriers. dHBV and wtHBV DNA were quanti-
fied by real-time PCR in the serum samples of patients either
infected with HBV alone (group 1; n⫽58) or coinfected with
HBV and HIV-1 (group 2; n⫽31) (table 1). To quantify
wtHBV DNA specifically, one of the primers was located inside
the intronic sequence, whereas, for dHBV DNA amplification,
one of the primers encompassed splice donor and acceptor
sites (figure 1A). The set of primers for dHBV was unable to
amplify wtHBV DNA plasmid, thus demonstrating the specific-
ity of these primers (data not shown). All samples tested were
positive for wtHBV DNA, with mean ⫾SE viral loads of
1.7 ⫻108⫾0.5 ⫻108and 1.1 ⫻108⫾0.3 ⫻108copies/mL
in groups 1 and 2, respectively (figure 1B). The level of
dHBV DNA was significantly lower than that of wtHBV DNA in
both groups. Defective viral DNA was detected in 73% of
samples (viral load 肁500 copies/mL), with means ⫾SEs
of 3.1 ⫻106⫾1.3 ⫻106and 10 ⫻106⫾7.9 ⫻106copies/
mL in groups 1 and 2, respectively (figure 1B).
Both dHBV and wtHBV DNA are generated from reverse
transcription of HBV pregenomic mRNA, either unspliced or
singly spliced [10 –16]. Thus, as expected, a correlation was ob-
served between the levels of dHBV and wtHBV DNA expression
for all patients (r⫽0.57; P⬍.0001) and in groups 1
(r⫽0.55; P⬍.0001) and 2 (r⫽0.54; P⫽.003) (figure 2A).
Strikingly, despite this correlation, defective particles were de-
tected in 2 of 12 patients with low replication (wtHBV load
⬍1⫻105copies/mL). In addition, in 14 of 77 patients with high
replication (wtHBV load ⬎1⫻105copies/mL), no dHBV par-
ticles were detected. These data suggest that dHBV expression is
related to more than just the level of HBV replication and raise
the question of the relationship between the regulation of HBV
splicing and viral liver disease.
Ratio of dHBV to total HBV particles in the serum of
chronic HBV carriers. To study dHBV expression indepen-
dent of viral replication, the ratio of dHBV DNA to total
(wtHBV plus dHBV) HBV DNA (dHBV/HBV ratio) was com-
pared for each patient. To take into account patients with unde-
tectable dHBV DNA, an arbitrary value of 50 copies/mL (10-fold
below the threshold of detection) was attributed. The dHBV/
HBV ratios were similar in both patient groups (for group 1,
mean ⫾SE of 4.8% ⫾1.2%, range of 0.001%–46% and me-
dian of 0.8%; for group 2, mean ⫾SE of 5.1% ⫾2.3%, range of
0.001%– 69%, and median of 1.3%; P⫽.29) (figure 2B). The
absence of a difference between the groups suggested that HIV-1
infection has no impact on HBV splicing events and the forma-
tion of defective particles. Thus, both HBV and HBV/HIV
groups were pooled to explore whether the variations observed
in dHBV/HBV ratios (from 0.001% to 69%) might be related to
HBV genetic status or liver disease.
The dHBV/HBV ratio and HBV status. HBV genotype and
mutations in the preC/C region have been implicated in the
modulation of viral replication and HBeAg expression [7, 28,
29]. Thus, we wanted to investigate whether viral genotype, mu-
tations in the preC/C region, and the level of HBeAg expression
were involved in the variation in the dHBV/HBV ratio. In our
cohort, 86% of the HBV samples belonged to HBV genotype A,
C, or E (figure 3A). Statistical analysis did not demonstrate a
difference when the dHBV/HBV ratio and HBV genotypes were
analyzed (figure 3A). For the preC G1896A stop codon and the
BCP A1762T and G1764A mutations, no significant difference
Figure 2. A, Relationship between the level of defective hepatitis B virus (dHBV) DNA and that of wild-type HBV (wtHBV) DNA in serum samples from 89
chronic HBV carriers. Black circles correspond to HBV/HIV-coinfected patients (group 2), and white circles correspond to HBV-monoinfected patients (group 1).
Values for wtHBV and dHBV loads were determined by real-time quantitative polymerase chain reaction and are represented using logarithmic scales. When
dHBV DNA was undetectable, an arbitrary value of 50 copies/mL (10-fold below the threshold of detection) was attributed. B, Box plot of the distribution of
the dHBV/HBV ratios (i.e., the ratio of dHBV DNA to total [wtHBV plus dHBV {wt⫹d}] HBV DNA) in groups 1 and 2. Ratios are expressed as percentages.
Defective HBV Particles and Liver Disease ●JID 2008:198 (15 July) ●221

was observed when the dHBV/HBV ratios were compared
(figure 3Band 3C). Finally, the dHBV/HBV ratio was not sig-
nificantly different between HBeAg-positive (mean ⫾
SE, 4.0% ⫾1.3%; median, 1.3%) and HBeAg-negative (mean
⫾SE, 6.2% ⫾2.1%; median, 0.5%) patients (P⫽.59) (figure
3D). These data suggest that the dHBV/HBV ratio is not influ-
enced by mutations usually involved in the modulation of HBV
replication.
The dHBV/HBV ratio and liver disease. The next step was
to study the relationship between HBV-associated liver diseases and
the dHBV/HBV ratio. No significant difference could be seen in
the dHBV/HBV ratio according to ALT activity (for ALT level less
than twice the normal value, mean ⫾SE of 3.2% ⫾0.7% and
median of 0.7%; for ALT level more than or equal to twice the
normal value, mean ⫾SEof5.7% ⫾2.4% and median of 1.4%;
P⫽.71) (figure 4A). However, dHBV/HBV ratios were signif-
icantly higher in patients with severe fibrosis (mean ⫾SE,
8.1% ⫾2.3%; median, 1.8%) than in those with moderate fi-
brosis (mean ⫾SE, 2.2% ⫾0.5%; median, 0.9%) (P⫽.04)
(figure 4B). Furthermore, dHBV/HBV ratios were significantly
higher in the population with severe liver necrosis (mean ⫾SE,
7.6% ⫾2.1%; median, 1.8%) than in those with moderate or
no liver necrosis (mean ⫾SE, 1.8% ⫾0.6%; median, 0.3%)
(P⫽.009) (figure 4C). The 4-fold increase in mean dHBV/
HBV ratio in patients with severe liver necrosis was a conse-
quence of a 2-fold decrease in wtHBV load and a 2-fold in-
crease in dHBV load. However, no significant difference was
observed between patients with moderate or no liver necrosis and
those with severe liver necrosis for either wtHBV load (mean
⫾SE, 2.4 ⫻108⫾0.9 ⫻108and 0.9 ⫻108⫾0.3 ⫻108
copies/mL, respectively) or dHBV load (mean ⫾SE,
2.5 ⫻106⫾1.5 ⫻106and 6.2 ⫻106⫾4.6 ⫻106copies/
mL) (P⫽.64). Similar results were observed for fibrosis (data
not shown). Thus, our data support the notion of a specific reg-
ulation of dHBV expression according to the severity of liver
disease.
Figure 3. dHBV/HBV ratios (i.e., the ratio of defective hepatitis B virus [dHBV] DNA to total [wild-type HBV plus dHBV {wt⫹d}] HBV DNA) according
to viral status. Ratios are expressed as percentages. Panel A shows a box plot of dHBV/HBV ratios according to HBV genotype. HBV genotypes (A, B,
C, D, and E) were determined for 87 of 89 chronic HBV carriers on the basis of sequence analysis of the capsid gene. In our cohort, 86% of HBV samples
belonged to HBV genotypes A, C, or E. No significant difference was found between genotypes A, C, and E by analysis of variance. For HBV genotypes
B and D, recruitment was insufficient to allow for statistical analysis. Box plots are also shown for dHBV/HBV ratios as functions of the G1896A mutation
(mut) in the precore/core sequence (B), of the basal core promoter (BCP) A1762T and G1764A mutations (C), and of hepatitis B e antigen (HBeAg)
expression (D). Statistical analysis was performed with the nonparametric Mann-Whitney Utest. Neg, negative; Pos, positive.
222 ●JID 2008:198 (15 July) ●Soussan et al.
 6
7
8
6
7
8
1
/
8
100%