HBcrAg vs HBsAg for Hepatitis B Inactive Carrier ID
Telechargé par
Idriss Lahlou Amine

Original article
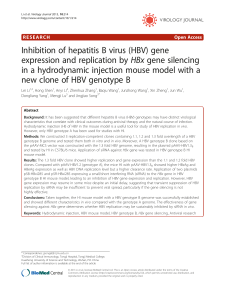
Serum hepatitis B core-related antigen is more accurate than hepatitis
B surface antigen to identify inactive carriers, regardless of hepatitis B
virus genotype
M. Riveiro-Barciela
1
,
2
,
*
, M. Bes
2
,
3
, F. Rodríguez-Frías
2
,
4
, D. Tabernero
2
,
4
,A.Ruiz
2
,
4
,
R. Casillas
5
, J. Vidal-Gonz
alez
1
, M. Homs
2
,
4
, L. Nieto
4
, S. Sauleda
2
,
3
, R. Esteban
1
,
2
,
M. Buti
1
,
2
1)
Liver Unit, Department of Internal Medicine, Hospital Universitari Vall d'Hebron and Universitat Aut
onoma de Barcelona, Barcelona, Spain
2)
Centro de Investigaci
on Biom
edica en Red de Enfermedades Hep
aticas y Digestivas (CIBERehd), Instituto de Salud Carlos III, Madrid, Spain
3)
Transfusion Safety Laboratory, Banc de Sang i Teixits, Servei Catal
a de la Salut, Barcelona, Spain
4)
Liver Pathology Unit, Departments of Biochemistry and Microbiology (Virology Unit) Hospital Universitari Vall d'Hebron and Universitat Aut
onoma de
Barcelona, Barcelona, Spain
5)
Vall d'Hebron Institut de Recerca, Barcelona, Spain
article info
Article history:
Received 12 September 2016
Received in revised form
24 February 2017
Accepted 5 March 2017
Available online 11 March 2017
Editor: G. Antonelli
Keywords:
HBcrAg
HBeAg negative chronic hepatitis B
HBsAg
HBV inactive carrier
Hepatitis B
Hepatitis B virus genotype
abstract
Objectives: To investigate whether hepatitis B surface antigen (HBsAg) and hepatitis B core-related an-
tigen (HBcrAg) levels are useful to identify inactive carriers among HBeAg-negative patients infected by
different hepatitis B virus (HBV) genotypes.
Methods: In all, 202 consecutive HBeAg-negative patients with chronic hepatitis B, 135 inactive carriers
and 67 with HBV activity, were prospectively followed for 1 year.
Results: In HBeAg-negative patients, HBsAg levels differed across the different genotypes (p <0.001). The
highest levels were observed in genotypes F or H (4.2 ±0.6 logIU/mL), followed by genotype E
(3.4 ±1.1 logIU/mL), genotype A (3.4 ±0.8 logIU/mL), and the lowest in genotype D (2.7 ±1.1 logIU/mL).
Variations in HBsAg levels were similar in inactive carriers and patients with HBV activity. HBsAg
<3 logIU/mL showed good performance for identifying genotype D inactive carriers: 76% of genotype D
inactive carriers met this cut-off versus 31% for genotypes A, E, F or H. However, in patients with ge-
notype A, HBsAg levels 3.7 logIU/mL better classified inactive carriers. The combination of a single
measurement of HBcrAg 3 logU/mL plus HBV DNA 2000 IU/mL yielded a positive predictive value and
diagnostic accuracy >85% in all HBV genotypes, except genotype H or F, with values of 62.5% and 72.7%,
respectively, for the two parameters.
Conclusions: HBsAg levels varied across genotypes in HBeAg-negative patients. HBsAg levels <3 logIU/mL
were only useful for identifying genotype D inactive carriers. A single HBcrAg measurement 3 logU/mL
plus HBV DNA 2000 IU/mL was highly accurate for identifying inactive carriers, regardless of their HBV
genotype. M. Riveiro-Barciela, Clin Microbiol Infect 2017;23:860
©2017 European Society of Clinical Microbiology and Infectious Diseases. Published by Elsevier Ltd. All
rights reserved.
Introduction
Hepatitis B e antigen (HBeAg) -negative chronic hepatitis B
(CHB) infection is the most common form of hepatitis B virus (HBV)
infection in many countries, including southern Europe [1,2]. One of
the most challenging issues in CHB is to distinguish between the
active HBeAg-negative phase of the infection and the inactive car-
rier state. The prognosis of the disease and the indication for
therapy differ in these two clinical situations; hence, their differ-
entiation is crucial. Therapy is not recommended in HBeAg-
negative inactive carriers, and monitoring can be reduced
because of their favourable long-term prognosis. In contrast,
HBeAg-negative patients with HBV activity have a higher risk of
*Corresponding author. M. Riveiro-Barciela, Hospital Universitari Vall d'Hebron,
Passeig Vall Hebron, 119-129, 08035, Barcelona, Spain.
E-mail address: mar[email protected] (M. Riveiro-arciela).
Contents lists available at ScienceDirect
Clinical Microbiology and Infection
journal homepage: www.clinicalmicrobiologyandinfection.com
http://dx.doi.org/10.1016/j.cmi.2017.03.003
1198-743X/©2017 European Society of Clinical Microbiology and Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
Clinical Microbiology and Infection 23 (2017) 860e867

developing liver fibrosis and hepatocellular carcinoma, so regular
monitoring and, in many cases, antiviral therapy are needed. To
accurately identify inactive carrier status, the current guidelines
recommend at least three alanine aminotransferase (ALT) and HBV
DNA determinations during 1 year.
Since Blumberg's discovery of hepatitis B surface antigen
(HBsAg) in 1965, this parameter has been accepted as a laboratory
marker to establish HBV infection [3]. HBsAg production is
controlled, at least in part, by the amount of intrahepatic covalently
closed circular DNA and the specific host immune response against
the HBV envelope proteins. This is particularly evident in HBeAg-
positive patients who show a high correlation between covalently
closed circular DNA and HBsAg levels [4]. The amount of circulating
HBsAg varies during the different phases of chronic infection: levels
are higher in immunotolerant patients and they decrease after
HBeAg seroconversion, and levels are lower in inactive carriers than
in HBeAg-negative CHB patients [5e8]. For this reason, HBsAg
determination has been cited as a potentially useful tool to identify
inactive carriers [9]. Brunetto et al.[10] proposed a combination of
HBsAg level <3 logIU/mL plus HBV DNA 2000 IU/mL to identify
inactive carrier status at a single time-point in HBeAg-negative
patients. The reported diagnostic accuracy was 93%, but the
cohort was limited to genotype D-infected patients. Currently, ten
different HBV genotypes have been described, each with a char-
acteristic geographical distribution [11,12]: genotype A pre-
dominates in northern Europe and America, genotypes B and C in
Asia, genotype D in southern Europe, genotype E in Africa, and
genotypes H and F in South America [2,12]. Recently, hepatitis B
core-related antigen (HBcrAg) has emerged as a new serological
marker for CHB. As HBcrAg correlates well with intrahepatic
covalently closed circular DNA levels in both naïve patients and
those treated with nucleoside analogues [13,14], it may also be
useful for proper classification of HBeAg-negative patients.
The aim of this study was to investigate the performance of
HBsAg and HBcrAg determinations to categorize HBeAg-negative
patients across the various HBV genotypes.
Patients and methods
Patient selection and definitions
Consecutive treatment-naive HBeAg-negative patients chroni-
cally infected with HBV (HBsAg-positive for more than 6 months)
were prospectively selected in the outpatient clinics of a tertiary
hospital. According to the guidelines of the European Association
for the Study of the Liver [9], patients were classified as follows:
inactive carriers, persistently normal ALT levels and HBV DNA
2000 IU/mL in three determinations over 1 year; active carriers,
HBV DNA >20 000 IU/mL, or at least one fluctuation of HBV DNA
>2000 IU/mL plus abnormal ALT levels (above the upper limit of
normality). Patients were regarded as ‘intermediate’on HBV DNA
fluctuation between 2000 and 20 000 IU/mL regardless of ALT
levels within the year of follow up [15]. For the purposes of this
study, patients classified as either intermediate or active carriers
were analysed together as patients with HBV activity, as all had HBV
DNA >2000 IU/mL and therefore, a three-fold higher probability of
disease progression [9,16].
Patients were excluded if they had undergone liver trans-
plantation, were co-infected with hepatitis C virus, hepatitis D vi-
rus, or human immunodeficiency virus (HIV), had high alcohol
intake, evidence of liver cirrhosis based on ultrasound findings
(hepatic parenchyma nodules, spleen >12 cm, portal vein >16 mm),
or analytical data (platelet count persistently below 140 10E9/
mL). This study was conducted in accordance with the Declaration
of Helsinki guidelines and the principles of Good Practice, and
was approved by the Ethic Review Board of the Vall d'Hebron
Hospital.
Data acquisition
Data on demographics (sex, age and race) were prospectively
collected, and the clinical history was collected from the patients'
medical records at the time of enrolment. Data on chemistry (ALT,
aspartate aminotransferase (AST),
g
-glutamyl transferase, bilirubin,
and albumin), haematology (platelet count, prothrombin time), and
HBV serology and virology (serum HBsAg and HBcrAg, HBV DNA,
HBV genotype) were also collected.
Laboratory measurements
HBsAg was quantified using the COBAS 80000 HBsAg II assay
(Roche Diagnostics, Mannheim, Germany): lower limit of detec-
tion, 0.05 IU/mL. HBcrAg was quantified by an electro-
chemiluminescent assay: Lumipulse
®
GHBcrAg assay (Fujirebio,
Fujirebio Europe, Gent, Belgium): lower limit of detection, 2 logU/
mL. This technique simultaneously determines denatured HBeAg,
HBcAg and a 22-kDa precore protein (p22cr), as all three share an
identical sequence of 149 amino acids. Hepatitis C virus, hepatitis D
virus and HIV were detected by commercially available immuno-
assays. Serum HBV DNA was quantified by PCR with a COBAS 6800
HBV test (Roche Diagnostics): lower limit of quantification 20 IU/
mL, lower limit of detection 10 IU/mL. For HBV genotyping, HBV
DNA was first enriched by ultracentrifugation of 9.6 mL of serum.
Subsequently, Sanger sequencing was carried out after amplifica-
tion of two different viral regions: PreC/Core (nucleotides
1774e2389, 615 bp) and PreS/Surface (nucleotides 2828e176,
561 bp), as previously reported [17]. Phylogenetic analysis was
performed with HBV reference sequences using neighbour-joining
analysis with the MEGA program, version 6. Genotypes H and F
were combined due to their phylogenetic proximity and
geographic distribution in the same areas [18,19].
Statistical analysis
Normally distributed quantitative variables were compared
with the Student's ttest and expressed as the mean ±standard
deviation. Variables with a non-normal distribution were analysed
with the ManneWhitney Utest and expressed as the median and
interquartile range. Categorical variables were compared between
groups using the chi-squared or Fisher exact test, as appropriate.
Correlations were tested with the Spearman correlation test. The
diagnostic performance of HBsAg and HBcrAg levels was evaluated
by receiver operating characteristic curve analysis. The cut-off
value to differentiate inactive carriers from patients with HBV ac-
tivity was selected considering the highest Youden index. All sta-
tistical analyses were performed using IBM SPSS, 20 (SPSS Inc.,
Chicago, IL, USA).
Results
Baseline characteristics
Of the 213 consecutive treatment-naive HBeAg-negative pa-
tients evaluated, 202 were included: 135 (66.8%) were classified as
inactive carriers, 12 (6%) as active carriers, and 55 (27%) as in-
termediates (see Supplementary material, Fig. S1). Therefore, 67
individuals met the ‘HBV activity’criteria. Eleven patients (5.2%)
with HBV DNA <10 IU/mL were excluded because HBV genotype
could not be determined at this level.
M. Riveiro-Barciela et al. / Clinical Microbiology and Infection 23 (2017) 860e867 861

Baseline characteristics are summarized in Table 1 and in the
Supplementary material (Table S1). The predominant genotypes
were A (37%), D (29%), E (18%), and F or H (12%). Patients with HBV
activity were younger, and had higher ALT, HBV DNA, HBsAg and
HBcrAg levels than inactive carriers (Table 1). Distribution of HBV
genotypes was similar between inactive carriers and patients with
HBV activity (p 0.98). Overall, mean HBV DNA levels were similar
between the main genotypes (p 0.91). Univariate and multivariate
analyses of baseline characteristics between inactive carriers and
patients with HBV activity are summarized in the Supplementary
material (Table S2).
Serum HBsAg levels according to the phase of chronic hepatitis B
infection and HBV genotype
Overall, HBsAg levels were lower in inactive carriers than in
patients with HBV activity (p 0.003). HBsAg levels differed signifi-
cantly (p <0.001) across the HBV genotypes, being highest for ge-
notype F or H, followed by E, A, and the lowest, D (Table 2). When
HBsAg levels were compared between these two groups according
to HBV genotype, significant differences were only observed for
genotypes A and D (p 0.002 and p <0.001, respectively) (Fig. 1).
A positive correlation between HBsAg and HBV DNA was found
in patients with HBV genotype A (r 0.46, p <0.001) and D (r 0.56,
p<0.001) infection, but there were no correlations in genotypes E,
or F or H (Fig. 2a).
Serum HBcrAg levels according to the phase of chronic hepatitis B
infection and HBV genotype
HBcrAg levels varied among the HBV genotypes in patients with
HBV activity (p 0.02) (Table 2) and were similar in inactive carriers
(p 0.052) (see Supplementary material, Table S3). In the compari-
son of HBcrAg levels between inactive carriers and patients with
HBV activity according to genotype, differences were only observed
in genotype A-infected patients (Fig. 1). Correlations between
HBcrAg and HBV DNA were only observed in genotype A (r 0.43, p
<0.001), although there was a trend to a correlation in genotype E
patients (r 0.49, p 0.057) (Fig. 2b). All HBV genotype H and F pa-
tients had HBcrAg levels <2 logU/mL, the lower limit of detection,
which precluded the study of correlations.
There was a moderate correlation between HBsAg and HBcrAg
levels in patients with genotypes A (r 0.55, p <0.001) and D (r 0.41, p
0.01), and no correlations in genotype E, F or H infection (Fig. 2b).
HBsAg and HBcrAg levels to identify HBV inactive carriers
Overall, the area under the receiver operating characteristic
curve (AUC) for identification of inactive carrier status was 0.67
(95% CI 0.56e0.77; p 0.003) for HBcrAg and 0.63 (95% CI 0.55e0.71;
p 0.001) for HBsAg. The cut-off associated with the highest Youden
index was 3.21 logIU/mL for HBsAg (sensitivity 49.6%; specificity
77.6%) and 3 logU/mL for HBcrAg (sensitivity 97.84%; specificity
Table 1
Baseline characteristics according to the stage of HBV infection
Total (n¼202) Inactive carriers (n¼135) HBV activity (n¼67) p value
Age, years, median (IQR) 46 (36e56) 48 (39e57) 43 (32e54) 0.004
Male, n(%) 112 (55%) 81 (60%) 31(47%) 0.07
Genotype, n(%)
A 75 (37%) 52 (38%) 23 (34%) 0.98
B or C 5 (2%) 1 (1%) 4(6%)
D 58 (29%) 38 (28%) 20 (30%)
E 36 (18%) 26 (19%) 10 (15%)
F or H 24 (12%) 16 (12%) 8 (12%)
Mixed A/E 4 (2%) 2 (2%) 2 (3%)
ALT, IU/mL, median (IQR) 18 (13e28) 16 (11e24) 23 (16e33) <0.001
Platelets, 10E9/L, median (IQR) 225 (188e251) 222 (185e248) 227 (197e255) 0.25
Albumin, mg/dL, median (IQR) 4.4 (4.2e4.6) 4 (4.2e4.6) 4.4 (4.1e4.6) 0.81
HBsAg, logIU/mL, median (IQR) 3.5 (2.6e4.1) 3.3 (2.4e4.0) 3.7 (3.2e4.1) 0.003
HBcrAg, logU/mL, median (IQR)
a
2.0 (2e2.5) 2.0 (2.0e2.0) 2.0 (2.0e3.3) <0.001
HBV DNA, logIU/mL, median (IQR) 2.7 (2.1e3.3) 2.5 (1.9e2.9) 3.5 (3.0e3.8) <0.001
Abbreviations: ALT, alanine aminotransferase; HBcrAg, hepatitis B core-related antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; IQR, interquartile range.
a
Available in 134 patients.
Table 2
Comparison of HBsAg and HBcrAg levels according to HBV genotype and disease activity in HBV infection
Total GT A GT D GT E GT F or H p value
Total n202 75 58 36 24 d
HBsAg, logIU/mL, median (IQR) 3.5 (2.6e4.1) 3.5 (3.1e4.0) 2.7 (2.1e3.5) 3.7 (3.0e4.2) 4.3 (4.1e4.4) <0.001
HBcrAg, logU/mL, median (IQR) 2.0 (2.0e2.5) 2.0 (2.0e2.7) 2.0 (2.0e2.0) 2.0 (2.0e2.5) 2.0 (2.0e2.0) 0.052
Inactive carriers n(%) 135 (67%) 52 (39%) 38 (28%) 26 (19%) 16 (12%) d
HBsAg, logIU/mL, median (IQR)
a
3.3 (2.4e4.0) 2.7 (3.3e3.8) 2.4 (1.8e2.9) 3.7 (2.9e4.2) 4.3 (3.9e4.5) <0.001
HBcrAg, logU/mL, median (IQR)
b
2.0 (2.0e2.0) 2.0 (2.0e2.2) 2.0 (2.0e2.0) 2.0 (2.0e2.3) 2.0 (2.0e2.0) 0.63
HBV activity n(%) 67 (33%) 23 (34%) 20 (30%) 10 (15%) 8 (12%) d
HBsAg, logIU/mL, median (IQR)
c
3.7 (3.2e4.1) 3.8 (3.5e4.2) 3.4 (2.9e3.7) 3.8 (3.2e4.2) 4.3 (4.2e4.4) 0.003
HBcrAg, logU/mL, median (IQR)
d
2.0 (2.0e3.3) 2.9 (2.0e3.4) 2.0 (2.0e2.6) 2.0 (2.3e5.8) 2.0 (2.0e2.0) 0.02
Abbreviations: GT, genotype; HBcrAg, hepatitis B core-related antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; IQR, interquartile range.
a
HBsAg in inactive carriers: p <0.001 for genotype A versus D; p 0.57 for genotype A versus E; p <0.001 for genotype A versus F or H; p <0.001 for genotype D versus E;
p<0.001 for genotype D versus F or H; p 0.013 for genotype E versus F or H.
b
HBcrAg in inactive carriers: p 0.55 for genotype A versus D; p 0.75 for genotype A versus E; p 0.24 for genotype A versus F or H; p 0.52 for genotype D versus E; p 0.48 for
genotype D versus F or H; p 0.14 for genotype E versus F or H.
c
HBsAg in patients with HBV activity: p 0.02 for genotype A versus D; p 0.87 for genotype A versus E; p 0.06 for genotype A versus F or H; p 0.09 for genotype D versus E;
p<0.001 for genotype D versus F or H; p 0.07 for genotype E versus F or H.
d
HBcrAg in HBV activity: p 0.03 for genotype A versus D; p 0.94 for genotype A versus E; p 0.01 for genotype A versus F or H; p 0.34 for genotype D versus E; p 0.21 for
genotype D versus F or H; p 0.13 for genotype E versus F or H.
M. Riveiro-Barciela et al. / Clinical Microbiology and Infection 23 (2017) 860e867862

27.3%). In genotype A, the HBcrAg AUC was higher than that of
HBsAg (AUC 0.80, 95% CI 0.65e0.95; p <0.001, and AUC 0.73, 95% CI
0.60e0.85; p 0.002, respectively). In genotype D, only HBsAg
determination had sufficient discriminatory power to identify
inactive carriers (AUC 0.78, 95% CI 0.66e0.90; p <0.001). Higher
HBsAg levels in genotype A than genotype D-infected patients at
baseline resulted in different cut-offs to identify inactive carriers.
HBsAg <3 logIU/mL showed a diagnostic accuracy of 74.1% for ge-
notype D, but only 49.3% for genotype A (Table 3). The cut-off
showing the best performance in genotype A was HBsAg
3.7 logIU/mL (positive predictive value 82.2%; negative predictive
value 50%; diagnostic accuracy 69.3%). However, the previous cut-
offs were not useful for proper classification of inactive carriers
infected by other HBV genotypes (genotype E, AUC 0.57; p 0.48 and
genotype F or H, AUC 0.49; p 0.95).
The diagnostic accuracy of HBcrAg determination was higher
than that of HBsAg for identifying inactive carriers. A single HBV
DNA determination 2000 IU/mL together with HBcrAg 3 logU/
mL yielded a positive predictive value and diagnostic accuracy
>85% for all genotypes except H or F, which showed values of 63%
and 73%, for these two indexes, respectively (Table 3). Inclusion of
11 patients with undetectable HBV DNA in the cohort did not
change the diagnostic accuracy or predictive values of the above-
mentioned cut-offs (see Supplementary material, Table S4).
HBsAg determination with or without HBV DNA values did not
achieve higher diagnostic accuracy than the combined cut-offs of
HBcrAg 3 logU/mL plus HBV DNA 2000 IU/mL.
Variability of HBsAg levels
In total, 103 (51%) and 81 (40%) patients had consecutive
quantitative HBsAg determinations separated by 6 and 12 months,
respectively. The comparisons showed no differences in HBsAg
levels over this time period (month 6: mean difference 0.036, 95%
CI e0.035 to 0.11; p 0.32; month 12: mean difference 0.069, 95% CI
e0.024 to 0.16; p 0.15). In the comparison of consecutive HBsAg
levels in inactive carriers, 48 patients had at least two de-
terminations separated by 12 months, and a significant decay in
HBsAg levels was observed in this group (mean difference 0.16, 95%
CI 0.078e0.23; p <0.001). However, in the 33 patients with HBV
activity and an HBsAg follow up of at least 1 year, no changes were
observed (p 0.67).
Discussion
In this prospective study of well-classified HBeAg-negative pa-
tients infected by HBV genotypes A and D to F, we found consid-
erable variability in HBsAg levels across the genotypes, with
statistically higher levels in patients with genotype F or H, followed
by E, A and D. There was a high correlation between HBsAg and HBV
DNA levels in genotype A and D patients, which made HBsAg
quantification a good biomarker for proper identification of inac-
tive carriers infected by either of these genotypes. Our results
confirmed that the previously described HBsAg cut-off of <3 logIU/
mL [10] is particularly useful to identify genotype D inactive car-
riers, with a positive predictive value of 76% and diagnostic accu-
racy of 74%. These results stem from the low HBsAg levels in
patients with genotype D, the genotype associated with the lowest
levels (mean 2.7 logIU/mL). In the remaining HBV genotypes, the
percentage of inactive carriers who met this criterion was 31%, a
finding that indicates the need for HBV genotyping to use this
HBsAg cut-off value. For example, in genotype A patients, an HBsAg
value of 3.7 logIU/mL yielded the best performance for identifying
inactive carriers: positive predictive value 82% and diagnostic ac-
curacy 69%.
HBcrAg is a recently described serum marker formed by three
products from the preCore/Core gene that have an identical
sequence of 149 amino acids. As HBcrAg level decreases across the
different phases of chronic hepatitis B, it has been suggested as a
potential tool for identifying patients at risk of developing hepa-
tocellular carcinoma or HBV reactivation after discontinuing
nucleoside analogues [20,21]. Data are scarce on the possible role of
HBcrAg levels to help classify the chronic hepatitis B infection stage.
In our cohort, HBcrAg levels were associated with excellent pre-
dictive values for identifying HBV inactive carriers, in particular
when a single measurement of this biomarker was combined with
HBV DNA 2000 IU/mL. HBcrAg levels achieved higher diagnostic
accuracy for classifying inactive carriers across all the HBV
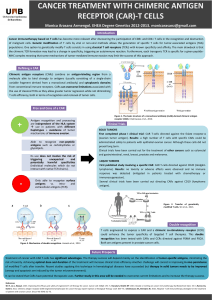
Fig. 1. Comparison of mean hepatitis B surface antigen (HBsAg) and hepatitis B core-related antigen (HBcrAg) levels between inactive carriers and patients with hepatitis B virus
(HBV) activity showed statistical differences in patients infected by genotype A (HBsAg and HBcrAg) and D (HBsAg), but not in those with genotypes E, F or H infection.
M. Riveiro-Barciela et al. / Clinical Microbiology and Infection 23 (2017) 860e867 863

genotypes than HBsAg quantification: a single HBV DNA determi-
nation 2000 IU/mL plus HBcrAg levels of 3 logU/mL showed an
overall positive predictive value and diagnostic accuracy of >85%.
There is extensive information concerning HBsAg levels in HBV
genotypes B and C [5,7,22e24]. However, data are scarce for ge-
notypes E to H, the most common genotypes in developing
countries, where HBV is more prevalent [18,19,25,26]. As HBV DNA
monitoring is not currently available worldwide [27], it would be
useful to have a serological marker that can identify inactive car-
riers in a single determination with less sophisticated technology
and easier manipulation and preservation of serum samples [9].
HBsAg quantification could be a good candidate, but the significant
Fig. 2. Correlations between hepatitis B virus (HBV) DNA and both hepatitis B surface antigen (HBsAg) (a) and hepatitis B core-related antigen (HBcrAg) (b) reached statistical
significance. Independent analysis by each genotype showed that correlations were only present in patients infected by genotype A (HBsAg and HBcrAg) and D (only HBsAg).
Moderate correlations between HBsAg and HBcrAg levels (c) were found in genotype A and D patients.
M. Riveiro-Barciela et al. / Clinical Microbiology and Infection 23 (2017) 860e867864
 6
7
8
6
7
8
1
/
8
100%