S2-1 NewDiagnosticTools_ProfFooks


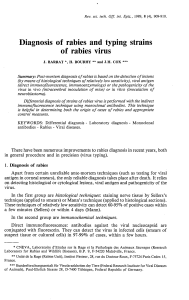
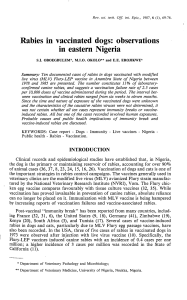
Overview
I. OIE resolutions
I. 1st International Conference on rabies in
Europe held in Kiev Ukraine - June 2005
II. Towards the Elimination of Rabies in Eurasia
held in Paris France - May 2007
II. Collection and storage of samples
III. OIE prescribed tests for rabies
IV. Alternative tests for rabies
iii. (non-prescribed)

1st International Conference on rabies in Europe (Kiev Ukraine - 2005)
Towards the Elimination of Rabies in Eurasia (Paris France - 2007)
Resolutions –rabies diagnosis:
•Clinical diagnosis of rabies is not reliable;
–A definitive diagnosis can only be made by laboratory investigations;
•OIE reference laboratories and WHO collaborating centres work together;
–International harmonisation of laboratory methods for diagnosis;
•The recommended primary diagnostic test for rabies is the fluorescent
antibody test;
–Confirmatory diagnosis, where required, should be undertaken using the rabies
tissue-culture infection test;
–The mouse inoculation test should only be used if tissue culture is not available;
–The use of the polymerase chain reaction and other amplification techniques is not
currently recommended for the routine diagnosis of rabies;
•Serological methods should not be used for routine rabies diagnosis;
–There is a requirement for rapid and accurate serological methods (i.e. ELISA
tests) to replace currently used virus neutralisation tests.
First International Conference on Rabies in Europe (2006) B. Dodet, A. Schudel, P-P. Pastoret, M. Lombard (eds).
Developments in Biologicals 125.
OIE Terrestrial Manual; WHO Laboratory Techniques in Rabies.

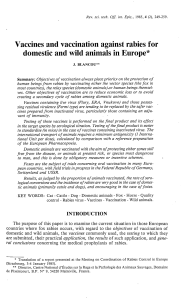
Rabies is an under-reported disease
•In a cohort of 133
children with CNS-
related diseases
–14 (10.5%) –rabies
•Three of 26 (11.5%)
clinically diagnosed
cases of cerebral
malaria were laboratory-
confirmed as rabies
Mallawa et al., 2007

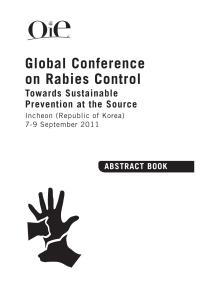
Objectives:
•Use of standardized diagnostic tests with regular inter-
laboratory tests in compliance with OIE standards
–Robust / Accurate
•High specificity / sensitivity
–Cheap
•Affordable
–Tests that do not involve the use of expensive
equipment / specialised laboratories
–Tests that are easy to use
•Tests that must be available and cost-effective for use
in rabies-endemic countries
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
1
/
40
100%





{kind=link}