TFG mrigovives poster

!
"#$%&'#!()$'$*+#,)!-"./!'$!+!,0#1'20#!34',4!+!#0(5+&!+50%#*!06!'#$%&'#!7(01%,)$!+!&03)(!)87),*)1!
9'0&0:',+&! ()$70#$)! +#1! '*! '$! +#! '570(*+#*! ,0570#)#*! 06! *4)! 7+*40:)#)$'$! 06! *;7)! ""! 1'+9)*)$!
5)&&'*%$! -<=/>! T4)! ".! ,+#! 0,,%(! $),0#1+(;! *0! 5+#;! ('$?! 6+,*0($! '#! 10:$! +#1! ,+*$.# T4)! ,&'#',+&!
5+#'6)$*+20#! '$! +! 7)($'$*)#*! 4;7)(:&;,+)5'+>! @0! 1)*)(5'#)! *4)! ,+%$)! 06! ".! '$! #),)$$+(;! +#1#
)&'5'#+2#:!'*!4)&7$!*0!'57(0A)!*4)!1'+9)2,!,0#*(0&>!
• B)*! 6%(*4)(! '#! '#$%&'#! ()$'$*+#,)! )20&0:;! *0! 1)C#)! *4)!
#+*%()!06!*4)!%#,0#*(0&&)1!1'+9)2,>!
• <'$,%$$! *4)! +15'#'$*)()1! '#$%&'#! 10$)! *0! ,0#$'1)(! '#$%&'#!
()$'$*+#,)>!
• D#+&;E)!)$*+9&'$4)1!1'+:#0$'$!7(0*0,0&>!
Test# Ini*al#evalua*on#and#
monitoring#
If#insulin#resistance#is#
suspected# Diagnosis#
Blood glucose curve!Dog, Cat (consider stress)!
Diabetes Mellitus, UTI,
other complications !
Fructosamine!Dog, Cat!
Urianalysis + culture!Dog, Cat!
Biochemical analysis +
electrolites!Dog, Cat!
CBC!Dog, Cat!
FeLV/FIV!Cat (unknown status)!Immunosupression!
T4!Cat!Hyperthyroidism!
Thyroid panel (T4, FT4,
T3, TSH)!Dog, Cat!Hyper / hypothyroidims!
Progesterone!Dog (intact female)!Diestrus!
Adrenal function test!Dog!Hyperadrenocorticism!
Catecholamine (blood,
urine)!Dog!Pheocromocytoma!
Panreatic panel (TLI,
PLI)!Dog, Cat!Pancreatitis!
!
IGF-1 ± TC or MRI!Cat!Acromegaly!
Abdominal ultrasound!
Thoracic radiography!Dog, Cat!
Neoplasia, Heart
insufficiency, Renal
insufficiency!
Cobalamin/Folate ± @F"! Dog, Cat!
Bacterial overgrowth,
Pancreatic exocrine
insufficiency !
GHIH! J! H057&)*)! 9&001! ,0%#*K! L@"! J! L('#+(;! *(+,*! '#6),20#K! M)FNOM"N! J! M)&'#)! F)%?)5'+! N'(%$! OM)&'#)! "55%#01)C,')#,;! N'(%$K! @P! J! @4;(08'#K! M@P! J! M())!
@4;(08'#K! @Q! J! @(''010*4;(0#'#)K! @RS! J! @4;(0'1T$25%&+2#:! 40(50#)K! @F"! J! @(;7$'#T&'?)! '55%#0()+,2A'*;K! UF"! J! U+#,()+2,! F'7+$)! '55%#0()+,2A'*;K! "BMTV! J!
"#$%&'#!&'?)TB(03*4!M+,*0(!VK!@H!J!H057%*)1!*050:(+74;K!=."!J!=+:#)2,!()$0#+#,)!'5+:'#:!
Secondary to insulin!
- Poorly preserved insulin!
- Expired insulin!
- Diluted !
- Inappropriate administration!
- Poor absorption!
- Abnormal activity duration!
- Production of anti-insulin
antibodies!
Case management!
- Exercise, diet, inappropriate
insulin!
- Incorrect dose and insulin
adjustments!
- Incorrect interpretation of
laboratorial database!
Concurrent diseases
(endogenous)!
- Obesity!
- Diestrus!
- Hyperadrenocorticism!
- Hypothyroidism!
- Hyperthyroidism!
- Acromegaly!
- Chronic inflammatory conditions
(especially pancreatitis)!
- Glucagonoma!
- Pheocromocytoma!
- Hyperlipidaemia!
- Renal insufficiency!
- Heart insufficiency!
- Diabetogenic drugs!
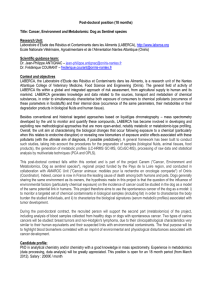
Hormones Associated disease Mechanism of insulin resistance
Progesterone
Exogenous
administration
Diestrus
Decreased receptor affinity for insulin
Reduced glucose transport in tissues
Growth hormone
(GH) Acromegaly
Decreased nº insulin receptors
Inhibited glucose transport
Increased lipolysis
Glucocorticoids
Exogenous
administration
Hyperadrenocorticism
Decreased receptor affinity for insulin
Decreased nº and affinity glucose transporters
Decreased glucose use in tissues
Increased hepatic gluconeogenesis
Thyroid hormones
Hyperthyroidism
Decreased insulin production
Decreased receptor affinity for insulin
Increased non-functional pro-insulin
Hypothyroidism
Post-receptor defect
Impaired glucose transport
Glucagon Pancreatitis
Bacterial infection
Activation hepatic glycogenolysis
Increased hepatic gluconeogenesis
Epinephrine Pheocromocytoma
Increased hepatic and renal gluconeogenesis
Mobilization of gluconeogenic precursors
Lipolysis to muscular tissue
Decreased insulin production
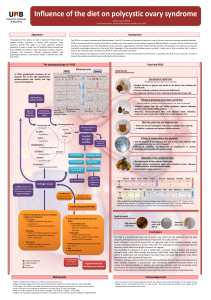
@4)! 50$*! ,0550#! ,+%$)! 06! ".! '#! 10:$! '$!
4;7)(+1()#0,0(2,'$5W! +#1! '#! ,+*$! '$! +,(05):+&;>!
"1)#2C,+20#! 06! ".! ()X%'()$! )&'5'#+20#! 06!
7(09&)5$! +$$0,'+*)1! 3'*4! *4)! '#$%&'#! '*$)&6! 0(!
03#)(! +15'#'$*(+20#! 06! '#$%&'#>! "*! '$! 70$$'9&)! *0!
1'A'1)! *4)! ,+%$)$! '#*0! )80:)#0%$! +#1!
)#10:)#0%$!-*+9&)!V/>!
!
Y#10:)#0%$!,+%$)$!+()!+$$0,'+*)1!3'*4!40(50#)T
5)1'+*)1! ".! 5),4+#'$5$! +#1! *4);! +()!
$%55+('E)1!'#!*+9&)!Z>!
@+9&)!V!
@+9&)!Z!
@+9&)!Q!
".! $40%&1! 9)! ,0#$'1)()1! '#! +! 10:! 0(! ,+*! 34)#! 50()!
*4+#!V>[!T!V>\!L"O]:!7)(!'#^),20#!06!'#$%&'#!'$!()X%'()1!
*0!5+'#*+'#!+1)X%+*)!:&;,)5',!,0#*(0&VWZ>!
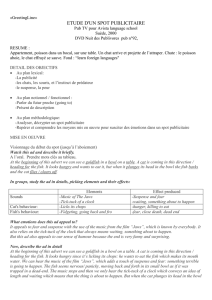
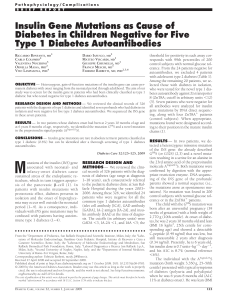
Figure# 1>! R)('+&! 9&001! :&%,0$)! 5)+$%()5)#*$! 7&0_)1! +:+'#$*! 25)>! @4)!
,0#,)#*(+20#!06!9&001!:&%,0$)!$*+;$!+90A)!V\[!5:O1&!+`)(!'#$%&'#!+15'#'$*(+20#W!
'#1',+2A)!06!".>!
• "#$%&'#! ()$'$*+#,)! ,+#! 0,,%(! +$! +! ()$%&*! 06! +#;! 7(0,)$$! *4+*! +&*)($! *4)! +A+'&+9'&'*;! 0(! +,20#! 06! '#$%&'#>! H+%$)$! ,+#! 9)! ,&+$$'C)1! '#*0! )80:)#0%$! +#1! )#10:)#0%$>! @4)!
)80:)#0%$!,+%$)$!+()!()&+*)1!*0!*4)!5'$5+#+:)5)#*!06!*4)!,+$)!9;!*4)!A)*)('#+('+#!0(!*4)!03#)(!+#1!$),0#1+(;!*0!'#$%&'#!'*$)&6>!@4)!)#10:)#0%$!,+%$)$!+()!()&+*)1!*0!
,0#,%(()#*!$'*%+20#$!0(!1'$)+$)$!'#!10:$!+#1!,+*$!$%,4!+$a!09)$'*;W!4;7)(!+#1!4;70*4;(0'1'$5W!1')$*(%$W!1'+9)*0:)#',!1(%:$W!9+,*)('+&!'#6),20#W!#)07&+$'+W!7+#,()+22$W!
()#+&!+#1!,+(1'0A+$,%&+(!'#$%b,')#,;K!9)'#:!4;7)(+1()#0,0(2,'$5!*4)!50$*!,0550#!,+%$)!06!".!'#!10:$W!+#1!+,(05):+&;!'#!,+*$>!D&&!*4)$)!7(0,)$$)$!4+A)!'#!,0550#!!
*4)!()&)+$)!06!40(50#)$!34',4!+&*)(!*4)!50&),%&+(!5),4+#'$5$!06!'#$%&'#!+#1!:&%,0$)!+,2#:!+*!7()T(),)7*0(W!(),)7*0(!+#1!70$*T(),)7*0(!&)A)&$>!
• M%(*4)(!$*%1')$!+()!#))1)1!*0!1)C#)!+!,&)+(!10$)!06!'#$%&'#!*0!1)*)(5'#)!()$'$*+#,)>!"*!1)7)#1$!0#!*4)!%#1)(&;'#:!,+%$)>!!
• @4)!1'+:#0$'$!7(0*0,0&!06!'#$%&'#!()$'$*+#,)!()X%'()$!+!1)*+'&)1!+#+5#)$'$W!,&'#',+&!4'$*0(;!+#1!+!74;$',+&!)8+5'#+20#>!@4)!9&001!:&%,0$)!,%(A)!'$!*4)!50$*!+77(07('+*)!
*00&!*0!1)*)(5'#)!*4)!*(%)!'#$%&'#!()$'$*+#,)>!R7),'C,!&+90(+*0('+&!*)$*$!60(!)+,4!,0#,%(()#*!1'$)+$)!+&&03!*0!)$*+9&'$4!+!1)C#'2A)!1'+:#0$'$>!D,4')A'#:!*4'$!1'+:#0$'$!'$!
'570(*+#*!*0!*()+*!*4)!,+%$)!+#1!'57(0A)!1'+9)2,!,0#*(0&>!
U)(60(5! +! 9&001! :&%,0$)! ,%(A)! '$! #),)$$+(;! *0!
1)*)(5'#)!+!*(%)!'#$%&'#!()$'$*+#,)>!M':%()!V!9)&0#:$!
*0! +! c! ;)+($! 0&1! #)%*)()1! 5+&)! 06! d0(?$4'()! *)((')(!
3'*4! <=! 1'+:#0$)1! e! 50#*4$! +:0>! @0! ,0#C(5! *4)!
,+%$)! +! &+90(+*0('+&! *)$2#:! +#1! '5+:'#:! 5%$*! 9)!
5+1)!-'&&%$*(+*)1!'#!*+9&)!Q/>!
V> M)&15+#!YHW!f)&$0#!.g>!H+#'#)!+#1!M)&'#)!Y#10,('#0&0:;!+#1!.)7(01%,20#>!Q1!)1>!R*>!F0%'$W!R+%#1)($W!Z[[P>!!
Z> S)$$!.R>!"#$%&'#!.)$'$*+#,)!'#!<0:$>!N)*!H&'#!f0(*4!D5!T!R5+&&!D#'5!U(+,*>!Y&$)A')(!F*1K!Z[V[KP[-Z/aQ[hiVe>!!
=+('+!1)&!=+(!.':0!N'A)$!
B(+%!)#!N)*)('#j('+!
I)&&+*)((+W!k%#)!Z[Ve!
1
/
1
100%