therapy-specific side effects of aromatase inhibi-

Corr espondence
n engl j med 375;16 nejm.org October 20, 2016
1591
therapy-specific side effects of aromatase inhibi-
tors are not discussed in their article.
Clemens Tempfer, M.D.
Ruhr University Bochum
Bochum, Germany
clemens . tempfer@ rub . de
No potential conf lict of interest relevant to this letter was re-
ported.
1. Spagnolo F, Sestak I, Howell A, Forbes JF, Cuzick J. Anastro-
zole-induced carpal tunnel syndrome: results from the Interna-
tional Breast Cancer Intervention Study II Prevention Trial. J Clin
Oncol 2016; 34: 139-43.
2. Lombard JM, Zdenkowski N, Wells K, et al. Aromatase in-
hibitor induced musculoskeletal syndrome: a significant prob-
lem with limited treatment options. Support Care Cancer 2016;
24: 2139-46.
DOI: 10.1056/NEJMc1610719
The authors reply: The MA.17R trial showed
that the rates of recurrent and contralateral
breast cancer were significantly lower among
women receiving extended aromatase-inhibitor
therapy than among those receiving placebo, al-
though the absolute differences were small. As
stated in our article, this benefit is likely to vary
according to the risk of recurrence of breast can-
cer. In our article, we conclude that the decision
to receive prolonged therapy with an aromatase
inhibitor (i.e., on the basis of the individual risk-
to-benefit ratio, or what Sanz and del Valle call “a
real benefit”) will depend on an individualized
assessment of quality of life during receipt of
therapy, the side-effect profile (particularly re-
lated to bone health), and the estimated risk of
disease recurrence. We believe that for patients
who have a high risk of recurrence, have had no
unacceptable side effects with previous aroma-
tase-inhibitor therapy, and have sufficient bone
health, prolonged therapy with an aromatase in-
hibitor should be discussed as a treatment option.
At the time of the initiation of the trial, aroma-
tase-inhibitor–associated carpal tunnel syndrome
and aromatase-inhibitor–induced musculoskele-
tal syndrome were not identified as adverse events
of interest in patients treated with an aromatase
inhibitor.1,2 In addition, the method used to as-
sess toxic effects in the trial (National Cancer
Institute Common Toxicity Criteria, version 2.0)
did not include these events as specific adverse
events. However, our data showed no significant
differences in grade 3 or 4 arthritis, muscle weak-
ness, or myositis between the letrozole group
and the placebo group. Similarly, no significant
between-group differences were detected with
respect to the adverse events of memory loss or
cognitive disturbance. As noted in our article,
the low incidence of adverse events with letro-
zole and the acceptable side-effect profile of the
drug, as compared with placebo, were probably
due to self-selection of study participants who
had had no unacceptable side effects during the
previous 5 years during which they had received
aromatase-inhibitor therapy and who were thus
willing to undergo another 5 years of treatment.
Therefore, we believe that the MA.17R trial cohort
is not comparable to the International Breast
Cancer Intervention Study II cohort, which com-
prised healthy, postmenopausal women with no
prior exposure to aromatase inhibitors.
James N. Ingle, M.D.
Mayo Clinic
Rochester, MN
Wendy R. Parulekar, M.D.
Queen’s University
Kingston, ON, Canada
wparulekar@ ctg . queensu . ca
Since publication of their article, the authors report no fur-
ther potential conf lict of interest.
1. Spagnolo F, Sestak I, Howell A, Forbes JF, Cuzick J. Anastro-
zole-induced carpal tunnel syndrome: results from the Interna-
tional Breast Cancer Intervention Study II Prevention Trial. J Clin
Oncol 2016; 34: 139-43.
2. Lombard JM, Zdenkowski N, Wells K, et al. Aromatase in-
hibitor induced musculoskeletal syndrome: a significant prob-
lem with limited treatment options. Support Care Cancer 2016;
24: 2139-46.
DOI: 10.1056/NEJMc1610719
Adaptive Randomization of Neratinib in Early Breast Cancer
To the Editor: The I-SPY 2 TRIAL (Investigation
of Serial Studies to Predict Your Therapeutic Re-
sponse with Imaging and Molecular Analysis 2)
uses adaptive randomization, putting more pa-
tients in the treatment group with the current
higher rate of pathological complete response. In
their Perspective article, Harrington and Parmi-
giani (July 7 issue)1 state that adaptive random-
ization makes more sense than fixed randomi-
zation. Why? Adaptive randomization is neither
The New England Journal of Medicine
Downloaded from nejm.org by andre Tartar on October 20, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

The new england journal of medicine
n engl j med 375;16 nejm.org October 20, 2016
1592
ethically nor statistically preferable. Randomiza-
tion requires equipoise.2 As long as equipoise ex-
ists, there is no logical or ethical reason to favor
one treatment over the other, and any assign-
ment ratio is acceptable, whether balanced (1:1)
or unbalanced (e.g., 2:1). The latter is used merely
to expose more patients to an experimental treat-
ment than to a well-known control. Ethically,
adaptive randomization is questionable if it is
used to lure patients into accepting trial partici-
pation on account of a higher probability of re-
ceiving a treatment of no proven benefit.3 Statis-
tically, adaptive randomization may bias the
treatment comparison, undermining the purpose
of randomization. The I-SPY 2 platform has cre-
ated a collaborative culture and proposed many
innovative ideas that may make future trials more
efficient.4 However, adaptive randomization is
not one of these ideas.
Marc Buyse, Sc.D.
Everardo D. Saad, M.D.
Tomasz Burzykowski, Ph.D.
International Drug Development Institute
Louvain-la-Neuve, Belgium
marc . buyse@ iddi . com
Drs. Buyse and Burzykowski report being employed by and
holding stock in the International Drug Development Institute,
and Dr. Saad reports being employed by the International Drug
Development Institute. No other potential conf lict of interest
relevant to this letter was reported.
1. Harrington D, Parmigiani G. I-SPY 2 — a glimpse of the
future of phase 2 drug development? N Engl J Med 2016; 375: 7-9.
2. Freedman B. Equipoise and the ethics of clinical research.
N Engl J Med 1987; 317: 141-5.
3. Hey SP, Kimmelman J. Are outcome-adaptive allocation trials
ethical? Clin Trials 2015; 12: 102-6.
4. Carey LA, Winer EP. I-SPY 2 — toward more rapid progress
in breast cancer treatment. N Engl J Med 2016; 375: 83-4.
DOI: 10.1056/NEJMc1609993
To the Editor: Park et al. (July 7 issue)1 report
that neoadjuvant neratinib plus weekly paclitaxel
resulted in a higher estimated rate of pathologi-
cal complete response than trastuzumab plus
weekly paclitaxel (56% vs. 33%), each followed by
four cycles of doxorubicin plus cyclophospha-
mide, in patients with human epidermal growth
factor receptor 2 (HER2)–positive, hormone-recep-
tor–negative breast cancer in the I-SPY 2 trial.
Curiously, when the same neoadjuvant chemo-
therapy regimens were investigated in another
randomized trial (the National Surgical Adjuvant
Breast and Bowel Project [NSABP] FB-7 trial) in
roughly similar patients with HER2-positive,
hormone-receptor–negative cancer, the rate of
pathological complete response was approximate-
ly similar with neratinib plus weekly paclitaxel
(46%) but substantially higher with trastuzumab
plus weekly paclitaxel (57%), the latter value be-
ing above the upper boundary of the 95% proba-
bility interval in the I-SPY 2 trial (11 to 54%).2
Few patients were treated with trastuzumab plus
weekly paclitaxel in each trial in this subgroup
and still fewer had a pathological complete re-
sponse (how many in the I-SPY 2 trial?). Besides
the slight differences between the trials, chance
might also in part explain these seemingly quite
different rates of pathological complete response
in the control (trastuzumab plus weekly pacli-
taxel) groups.
Heikki Joensuu, M.D.
Helsinki University Hospital
Helsinki, Finland
heikki . joensuu@ hus . fi
No potential conf lict of interest relevant to this letter was re-
ported.
1. Park JW, Liu MC, Yee D, et al. Adaptive randomization of
neratinib in early breast cancer. N Engl J Med 2016; 375: 11-22.
2. Jacobs SA, Robidoux A, Garcia JMP, et al. NSABP FB-7:
a phase II randomized trial evaluating neoadjuvant therapy with
weekly paclitaxel (P) plus neratinib (N) or trastuzumab (T) or
neratinib and trastuzumab (N+T) followed by doxorubicin and
cyclophosphamide (AC) with postoperative T in women with
locally advanced HER2-positive breast cancer. Cancer Res 2016;
76 Suppl 4: PD5-04. abstract.
DOI: 10.1056/NEJMc1609993
Drs. Berry and Esserman reply: Buyse et al.
ask, Why adaptive randomization? The answer is
that it makes great sense ethically, statistically,
economically, scientifically, and logistically, es-
pecially in a platform trial. The I-SPY 2 trial con-
siders many patient subtypes and therapies. Adap-
tive randomization slows down and even stops
assignment to therapies that perform poorly de-
pending on subtype. Consider neratinib: in mid-
trial, neratinib was performing poorly for HER2-
negative tumors with a status of high-risk
category 1 on a 70-gene profile (independent of
hormone-receptor status). The members of the
data and safety monitoring board considered
stopping neratinib in these two subtypes — until
they learned that the adaptive-randomization al-
gorithm had already done so. The trial continued
without an amendment because the patients had
several good alternatives within the trial. Nera-
tinib did well in other subtypes and eventually
The New England Journal of Medicine
Downloaded from nejm.org by andre Tartar on October 20, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

Corr espondence
n engl j med 375;16 nejm.org October 20, 2016
1593
reached prespecified thresholds for efficacy in a
specific biomarker signature (“graduated”).
The I-SPY 2 trial is focused on patients. Be-
cause of adaptive randomization, 57% of 115 pa-
tients assigned to neratinib were HER2-positive,
as compared with only 28% of 78 patients who
were concurrently assigned to receive control
therapy. This focus means that trial participants
are more likely to receive better therapy than
with equal randomization. It is also beneficial
for future patients because better-performing
therapies move through the trial faster and esti-
mates of the efficacy are more precise in sub-
types that have a response. The larger sample
sizes within subtypes that have a response also
mitigate the effects of early false positive results,
and the Bayesian covariate analysis reduces such
biases still further.
Buyse et al. also raise the possibility that
adaptive randomization may cause patients to be
inappropriately attracted to participate in the
trial. Yet participants know that they cannot get
a better-performing therapy unless there is one
in the trial.
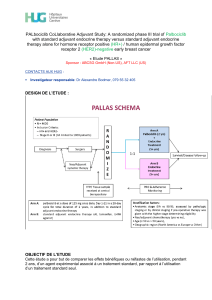
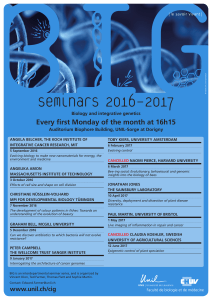
Joensuu asks about the differences in the es-
timated rates of pathological complete response
between the I-SPY 2 and FB-7 trials in the signa-
ture of neratinib in I-SPY 2 (Table 1 accompany-
ing this reply). The most obvious explanation is
variability in such estimates when sample sizes
are small, as he suggests. Indeed, the 57% rate
of pathological complete response in the FB-7
control group is based on eight such responses
in 14 patients, and the 46% rate in the neratinib
group is based on six such responses in 13 pa-
tients. The confidence intervals are wide. As in-
dicated in Table 1, these estimates are fragile
indeed. The probability intervals in the I-SPY 2
trial are wide as well.
Donald Berry, Ph.D.
M.D. Anderson Cancer Center
Houston, TX
Laura Esserman, M.D., M.B.A.
University of California, San Francisco
San Francisco, CA
laura . esserman@ ucsf . edu
Since publication of their article, the authors report no fur-
ther potential conf lict of interest.
DOI: 10.1056/NEJMc1609993
Drs. Harrington and Parmigiani reply: Buyse
and coauthors raise important questions about
adaptive randomization in the I-SPY 2 trial and in
clinical trials in general. We attempted to give a
balanced perspective on the strengths and limi-
tations of both adaptive and constant probability
designs, especially in Table 2 of our article (avail-
able at NEJM.org). We did not mean to imply that
adaptive randomization is always preferable; we
do believe that it can be an important tool for
trialists in settings in which many potential treat-
ments are emerging and there is identifiable pa-
tient heterogeneity. Potentially useful treatments
must be identified as soon as possible, and those
without promise should be quickly discarded.
Ethical standards underlying the enrollment
of patients into trials and the obtaining of in-
formed consent are very important and should
evolve with emerging paradigms of scientific
investigation. From a patient perspective, it seems
legitimate to consider the type of randomization
in deciding whether to enroll in a trial. For ex-
ample, a patient may prefer a trial with unbal-
anced randomization, in which more patients
are assigned to the experimental treatment. The
crux of the ethical issue is whether equipoise
should dictate balance. If one accepts unbalanced
randomization as ethical, then it follows that
presenting randomization properties to patients
is also ethically sound. Undoubtedly, presenting
this information effectively and impartially can
be a challenge. For example, in an unbalanced
design, it is also possible that more patients will
be exposed to serious side effects of an experi-
mental treatment that has no benefit. Although
adaptivity is ancillary to this ethical question, in
practice the complex nature of adaptation will
probably mean that the adaptation mechanism
will remain a black box to many patients, ampli-
fying the challenges of effective communication.
Trial
Rate of Pathological Complete Response
(95% CI or PI)
Control Neratinib
percent
NSABP FB-7 57 (31–83) 46 (19–73)
I-SPY 2 33 (11–54) 56 (37–73)
* CI denotes confidence interval, and PI probability interval.
Table 1. Efficacy among Patients with HER2-Positive,
Hormone-Receptor–Negative Breast Cancer in Two
Trials.*
The New England Journal of Medicine
Downloaded from nejm.org by andre Tartar on October 20, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

The new england journal of medicine
n engl j med 375;16 nejm.org October 20, 2016
1594
In a well-conducted multicenter trial with
adaptive randomization, the threat to clinical
equipoise is no different than in a standard fre-
quentist design with interim monitoring; the
accumulating results are not shared with inves-
tigators or patients who might participate. In a
single-center trial of two treatments, an adaptive
randomization might send a signal to participat-
ing investigators through the changing random-
ization fractions, but that is a situation in which
the use of adaptive randomization poses greater
challenges.
Standard summary statistics that are not ad-
justed for the adaptive randomization and the
changing mix of patients receiving a treatment
would, as Buyse et al. suggest, provide biased
estimates of treatment effects, and model-based
methods must be used. We raised that point as
well. The first question that we raise in the fifth
paragraph of our article points to the need to
learn more about the robustness of those methods.
David Harrington, Ph.D.
Giovanni Parmigiani, Ph.D.
Dana–Farber Cancer Institute
Boston, MA
Since publication of their article, the authors report no fur-
ther potential conf lict of interest.
DOI: 10.1056/NEJMc1609993
Meningococcal B Vaccine during a University Outbreak
To the Editor: Basta et al. (July 21 issue)1 mea-
sured protective serum antibody responses in col-
lege students immunized with a meningococcal
serogroup B vaccine (4CMenB) in response to an
outbreak. Although the vaccine elicited in vitro
protection against two reference strains, a third
of the students did not have a response with pro-
tective serum titers against the outbreak strain.
This result was unexpected on the basis of test
results from the Meningococcal Antigen Typing
System,2 which predicted susceptibility of the
outbreak strain to antibodies elicited by 4CMenB.
My colleagues and I previously investigated the
strain responsible for the outbreak.3 Despite high
expression of two vaccine antigens, factor H–
binding protein (fHbp) and neisserial heparin-
binding antigen, the strain was relatively resistant
to antibodies elicited in mice, nonhuman pri-
mates, and a human immunized with 4CMenB.
In other studies, meningococcal strains with simi-
lar expression of identical fHbp amino acid se-
quence variants had discordant susceptibility to
anti-fHbp bactericidal activity, which was related
to the greater ability of the resistant strain to bind
complement factor H, which down-regulates
complement.4 Collectively, the data underscore our
incomplete understanding of strain susceptibility
to vaccine-induced bactericidal activity, which lim-
its accurate prediction of vaccine coverage.
Dan M. Granoff, M.D.
UCSF Benioff Children’s Hospital Oakland
Oakland, CA
dgranoff@ chori . org
No potential conf lict of interest relevant to this letter was re-
ported.
1. Basta NE, Mahmoud AAF, Wolfson J, et al. Immunogenicity
of a meningococcal B vaccine during a university outbreak.
N Engl J Med 2016; 375: 220-8.
2. Donnelly J, Medini D, Boccadifuoco G, et al. Qualitative and
quantitative assessment of meningococcal antigens to evaluate
the potential strain coverage of protein-based vaccines. Proc
Natl Acad Sci USA 2010; 107: 19490-5.
3. Rossi R, Beernink PT, Giuntini S, Granoff DM. Susceptibil-
ity of meningococcal strains responsible for two serogroup B
outbreaks on U.S. university campuses to serum bactericidal
activity elicited by the MenB-4C vaccine. Clin Vaccine Immunol
2015; 22: 1227-34.
4. Giuntini S, Pajon R, Ram S, Granoff DM. Binding of comple-
ment factor H to PorB3 and NspA enhances resistance of Neis-
seria meningitidis to anti-factor H binding protein bactericidal
activity. Infect Immun 2015; 83: 1536-45.
DOI: 10.1056/NEJMc1610666
To the Editor: The article on immunogenicity
of meningococcal B vaccine during a university
outbreak showed that 66.1% of students vacci-
nated with the 4CMenB vaccine had serum bacte-
ricidal antibodies (SBA) against the outbreak
strain, in assays that included human comple-
ment (hSBA); 33.9% had a negative hSBA result.
The media incorrectly reported that one third of
students did not acquire immunity against the
outbreak strain.1 We want to point out that Gold-
schneider et al.2 established that although a pos-
itive result on hSBA assay indicates protection
against meningococcal disease, a negative hSBA
result is not an indication of susceptibility, be-
cause the assay result (positive vs. negative) under-
estimates immunity. Indeed, blood from people
The New England Journal of Medicine
Downloaded from nejm.org by andre Tartar on October 20, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
1
/
4
100%