Caracterización de la estadificación molecular en carcinoma de colon. Correlación clínico-histológica

Caracterización de la estadificación molecular
en carcinoma de colon. Correlación clínico-histológica
Iban Aldecoa Ansórregui
Aquesta tesi doctoral està subjecta a la llicència Reconeixement 3.0. Espanya de Creative
Commons.
Esta tesis doctoral está sujeta a la licencia Reconocimiento 3.0. España de Creative
Commons.
This doctoral thesis is licensed under the Creative Commons Attribution 3.0. Spain License.

P á g i n a | 63
Tesis Doctoral |Iban Aldecoa Ansorregui
TRABAJOS REALIZADOS,
MÉTODOS Y RESULTADOS

P á g i n a | 64
Tesis Doctoral |Iban Aldecoa Ansorregui

P á g i n a | 65
Tesis Doctoral |Iban Aldecoa Ansorregui
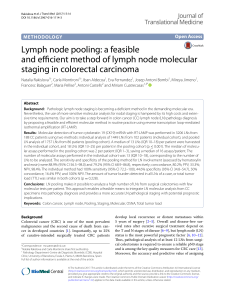
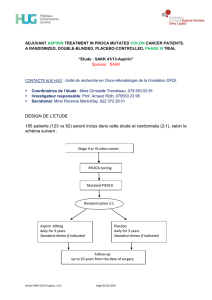
La descripción de los pacientes, la metodología utilizada así como los resultados encontrados
en las diferentes investigaciones realizadas, se encuentran detalladamente explicadas en las
secciones de “Materials and methods” y “Results” de cada uno de los dos artículos que constituyen
el cuerpo de la presente tesis doctoral.
Los dos artículos que se incluyen a continuación tal y como se encuentran en la literatura
científica.

P á g i n a | 66
Tesis Doctoral |Iban Aldecoa Ansorregui
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
1
/
39
100%