Centre Maladies Rares à Expressions

Centre référent ‘Maladies rares à
expression psychiatrique et
schizophrénies à début précoce’
Coordonateur : Pr David Cohen
Responsable: Dr Angèle Consoli, Dr Claudine Laurent
Psychologue: Antoine Tanet
Biostatistiques et data: Nicolas Bodeau Manager
Sandrine Cohen, Secrétariat
http://speapsl.aphp.fr

Introduction
•Seul centre référent psychiatrique en France
•Un champ d’actions large et couvrant des
pathologies très variées
•Une activité transversale et pluridisciplinaire par
nature
•Un axe principal : le diagnostic fonctionnel au service
des patients et des professionnels les prenant en
charge
•Une importante activité de publications
•Des recherches originales

Quelles activités ?
•Enfants, adolescents, jeunes adultes
•Consultations adressées par un médecin
•3 cas de figure avec recoupements
1. Pathologies psychiatriques atypiques avec suspicion de
maladie rare ou d’organicité
2. Maladies rares avec problématique psychiatrique
3. Schizophrénies à début précoce
•Recherche
•Diffusion / Sensibilisation
•Epidémiologie

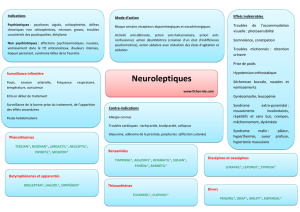
Quelles expressions psychiatriques
dans les maladies rares ?
•Pathologies psychiatriques spécifiques
–Schizophrénie
–Autisme, troubles envahissants du développement
–Trouble bipolaire, trouble de l’humeur, trouble anxieux,
hyperactivité / déficit de l’attention
•Retard Mental
•Troubles des apprentissages
•Troubles du comportement mal définis

Utilité du Centre référent
•Mauvaise définition des phénotypes
•Stratégies thérapeutiques complexes
•Reconnaissance de pathologies traitables sous
diagnostiquées dans pathologies psychiatriques
•Reconnaissance de troubles psychiatriques sous
diagnostiqués dans les pathologies rares et
organiques
•Sensibilisation des professionnels
•Question du diagnostic fonctionnel
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
1
/
43
100%