Les déficits immunitaires héréditaires et leurs thérapeutiques

Les déficits immunitaires héréditaires
et leurs thérapeutiques
C. Picard
Centre d’étude des déficits immunitaires
Déficits immunitaires héréditaires (DIH)
•Déficits immunitaires « classiques » :
> 200 déficits décrits, > 160 gènes décrits
1/5000 naissances
Classification :
•Déficits immunitaires combinés (T et B) (rares)
•Déficits immunitaires humoraux (B) (fréquents)
•Déficits de la phagocytose et de l’opsonisation
•Déficits de l’immunité innée
•Déficits de l’homéostasie du système immunitaire
•Pathologies auto-inflammatoires
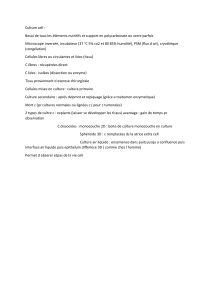
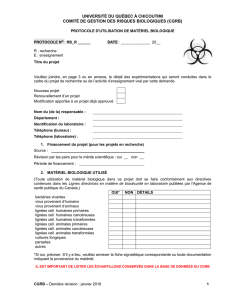
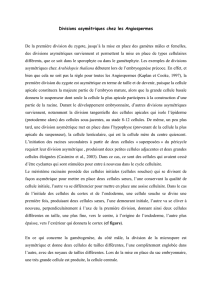
Déficit complet de l'immunité adaptative:
Déficit Immunitaire Combiné Sévère
CD8+ T cell
CD4+ T cell
NK cell
B cell
Common lymphoid
progenitor
Hematopoietic
stem cell
Common myeloid
progenitor
macrophage
dendritic cell
PMN
Déficit immunitaire combiné sévère (DICS)
Fréquence et transmission : 1/100 000, AR ou XR
Signes Cliniques = Infections
-opportunistes (Pneumocystose…)
- fongiques (Candidose…)
- virales (Parainfluenzae, Adv, CMV,VRS…)
- bactériennes, BCGite
Signes Biologiques et radiologiques :
- Absence de thymus
- Numération Formule Sanguine: lymphopénie < 1500/mm3
-LYMPHOCYTES T = 0
•Numération Formule Sanguine
lymphocytes +++
< 1500/mm3
•Absence de thymus
•Phénotypage lymphocytaire
absence de lymphocyte T
•Hypogammaglobulinémie
(hypoIgG, IgA et IgM)
Déficit immunitaire combiné sévère :
Diagnostic
1. Mort des thymocytes/lymphocytes (T-B-NK-):
→ déficit en adénosine déaminase (ADA), déficit en PNP et AK2
2. Défaut de signalisation cytokinique (T-B+):
→ IL2RG, IL7RA, JAK3
3. Défaut de réarrangement de VDJ (T-B-NK+):
→ RAG1, RAG2, Artémis, DNA-Pks, Cernunnos, DNA-Ligase 4
4. Anomalies du TCR ou du pré-TCR (T-):
→ CD45, CD3E,CD3D,CD3G, CD3Z, ZAP70
Déficit immunitaire combiné sévère :
4 mécanismes

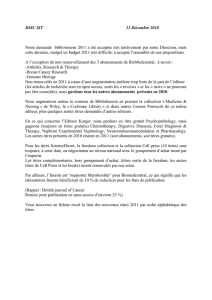
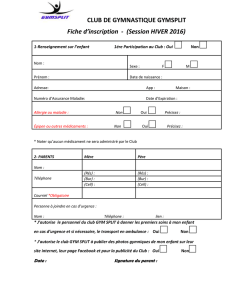
Déficit en adénosine déaminase (AR)
Enzyme ubiquitaire
Cellules ADA-déficientes = accumulation
•d-adénosine transformé par la deoxycytidine kinase (dCydK)
en:
•2'-deoxyadénosine 5'-triphosphate (d-ATP).
Ces 2 métabolites ont des effets sur le développement et la
fonction des lymphocytes (synthèse du DNA, blocage des
divisions cellulaires et de l’apoptose)
→ lymphopénie T, B et NK
DNA
d-Adénosine ↑
d-Inosine
ADA ↓
d-ATP ↑
d-CydK
X
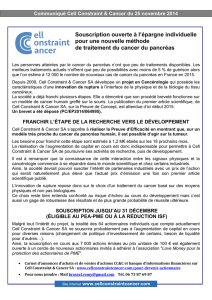
DICS par défaut de signalisation cytokinique
IL-2 IL-4 IL-7 IL-15 IL-21
gc
IL-9
T-lymphocyte development NK-lymphocyte development
gc gc gc gc gc
DICS T- B+ NK- XR (IL2RG):
DISC T-B+: IL7RA et JAK3 (AR)
Jak3 deficiency
T
CD4
NK
HSC
B
T
CD8
CLP IL-7
IL-2R,-4R,-7R,
-9R,-15R,-21R
Jak3
IL-7Ra
DICS T- B+ NK- AR (JAK3): DICS T- B+ NK+ AR (IL7RA):
gc gc
TcR: structure
Réarrangement
Recombinaison
D
V D J C
C
VDJ C
Configuration
réarrangée
2) Epissage
1) Recombinaison V(D)J
VJ
COOH
NH2
Vb
DbJb
Ja
Cb
Ca
Va Domaine
Variable
Domaine
Constant
s s
s
I
s
s
I
s
s
I
s
s
I
s
- II-
Reconnaissance de
la cassure d ’ADN
- I-
Initiation de la recombinaison:
RAG-1 et RAG-2
RSS
RSS
RAG-1 RAG-2
- III -
Réparation (NHEJ)
Artémis,Ligase IV et Cernunnos
DICS T-B-: anomalie de la recombinaison
Anomalies du TCR ou du préTCR
(CD45, CD3E,CD3D, CD3G, CD3Z, ZAP70) (AR)
Le Deist, médecine science 2007
XX
X
X
X
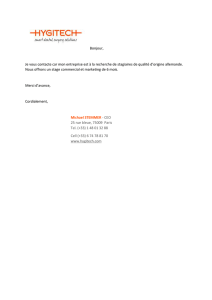
Déficit Immunitaire Combiné Sévère
CD8+ T cell
CD4+ T cell
NK cell
B cell
Common lymphoid
progenitor
Hematopoietic
stem cell
Common myeloid
progenitor macrophage
dendritic cell
PMN
Reticular
Dysgenesia
(AK2)
ADA
deficiency
SCID T-B+
(γ
γγ
γc,Jak3)
SCID T-B+NK+
IL7RA
SCID T-B-NK+
Rag1, Rag2, Artemis
CID T+/-B+NK+
CD3D,E,G,Z

Prise en charge thérapeutique
•Traitement anti-infectieux,antibioprophylaxie
•Immunoglobulines
•Traitement curatif:
–Greffe de cellules souches hématopoïétiques
•Geno-identique (fratrie)
•Phéno-identique (fichier)
•Haplo-identique (parents)
–Thérapie génique
(déficits en gammaC et ADA)
–Traitement substitutif (PEG-ADA)
Survival in SCID patients after related HLA-mismatched HSCT
according to year at grafting
european registry
Survival in SCID patients after related geno-id HSCT
Buckley Annu Rev Immunol 2004
Haplo identical HSCT for SCID as a function of years
of transplantation
< 1995 : 59%
> 1995 : 72%
P= 0.092
Survival rate
(10 years) %
survival
months
<1995 (n=128)
1995-2005 (n=94)
Kinetics of T cell developpment after HSCT
SCID with spontaneous reversion
= selective advantage of corrected T cells
Stephan V, et al. Atypical X-linked severe combined
immunodeficiency due to possible spontaneous reversion of the
genetic defect in T cells. N Engl J Med. 1996;335:1563-7.
Arredondo-Vega FX, et al. Adenosine deaminase deficiency with
mosaicism for a "second-site suppressor" of a splicing mutation:
decline in revertant T lymphocytes during enzyme replacement
therapy. Blood 2002 ;99:1005-13.
Hirschhorn R, e al. Spontaneous in vivo reversion to normal of an
inherited mutation in a patient with adenosine deaminase deficiency.
Nat Genet 1996; 13:290-5.

SCID with spontaneous reversion
= selective advantage of corrected T cells
Gene therapy for
Primary Immuno-deficiencies
Hematopoietic
Stem cells
Peripheral
Lymphocytes
Thymus
(2%)
(10%)
(10%)
Myeloid
lymphoid
progenitors
Reverted T cells
Mutated T cells
Gene therapy for SCID-X1/ The disease
*~ 60% of known SCID patients
*Lethal within one year of age
*Conventional therapy : HSCT
IL-2 IL-4 IL-7 IL-15 IL-21
gc
IL-9
T-lymphocyte development NK-lymphocyte development
gc gc gc gc gc
DICS T- B+ NK- XR (IL2RG):
Phase I/II ; No HLA-id donor
MLV-based retroviral vector
10 treated IL2RG deficient patients (March 1999- April 2002)
Age : 1-11 months (mean 7 months)
Infections : all
CD34 (+) γ
γγ
γc(+)/kg : 1-22 X 106 (median : 4.3x106/kg)
Transduction rate: 20-40%
Absence of Conditioning Regimen
F.U : 8- 11 years
SCID-X1 n°1 gene therapy trial
Full correction of T-cell immunodeficiency in 8 out of 10 patients
P9: - received 1 X 10-6 CD34 (+) γ
γγ
γc(+) / kg
- decline in immune function;
- HSCT 9/10 MUD 2 years post GT
- died from fungal pneumonia.
P3: - Failure after cell trapping in enlarged spleen;
- successful BMT = A.W
But 4 out of 8 patients developed acute T cell leukemia
Patients outcome
0
1000
2000
3000
4000
5000
6000
7000
0 1 2 3 4 5 6 7 8 9 10 11 12 13
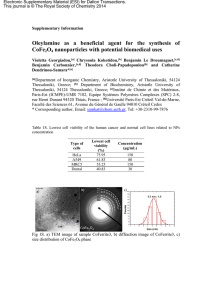
Early Kinetic of T cell reconstitution
CD34+gc+/kg
0
1000
2000
3000
4000
5000
6000
7000
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Months
CD3+ lymphocytes/µl
P1 : 3x106
P2 : 5x106
P6 : 1.2x106
P8 : 22x106
P4 : 18x106
P5 : 20x106
P7 : 4x106
P10 :11x106
P6
P2
P1
P8
P4
P5
P10
P7
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
0 20 40 60 80 100 120
Months
P2
P4
P8
P6 P1
P5
P7
P10
CD3+ lymphocytes/µl
Kinetic of T cell reconstitution

PBMC (41)
PBMC (81)
PBMC (97)
PBMC (64)
BV11
1,1 %
1,9 %
2,6 %
2,2 %
10 aa
10 aa
10 aa
10 aa
BV21
4,6 %
9,1 %
15 %
5,3 %
10 aa
10 aa
10 aa
10 aa
BV2
7,4 %
12,1%
10 aa
10 aa
10 aa
10 aa
11,7 %
6,6 %
10 aa
10 aa
10 aa
10 aa
BV6b
7,1 %
4 %
7,8 %
4,4 %
BV22
4,5 %
10,5 %
9,8 %
7 %
10 aa
10 aa
10 aa
10 aa
Thymic output
P2
0,1
1
10
100
1000
10000
0 20 40 60 80 100 120
P6
P8
P2
P1
P4
P5
P10
P7
TRECs/ 105PBMC
Months
Kinetics of Igs levels
0
400
800
1200
1600
0 20 40 60 80 100 120
P1
P2
P4
P8
P5
P7
0
100
200
300
400
500
0 20 40 60 80 100 120
P1
P2
P8
P7
P5
IgA
0
100
200
300
400
500
0 20 40 60 80 100 120
P1
P2
P8
P7
P5
IgM
IgG
Sequential Immunoscope Study of
T Vδ
δδ
δ1 Population
M23
M27
M31
M34
T g/d
control
M13
M17
3‘LTR
6 3113 2417 34 -C 37 M
**** * *
198 pbs
Monoclonal γδ
γδγδ
γδ T cell clone (immunoscope + TCR sequence)
Blast like cell but mature T cell phenotype
Integration site increased at least from m13
Patient 4 Clonality study
Longitudinal analysis
of vector integration sites
M6
Insertional mutagenesis /LTR driven oncogene activation
P4 (M+30), P5 (M+34) , P10 (M+33) and P7 (M+68)
1 2 34 5 6
MFG cMFG c
P5 P4 P10
CCND2
2.440 pb
MFG c
Intergenic, chr12p13.32
148
MFG cBMI1
25.240 pb
49.499 pb SPAG6, chr10p12.31
LMO2, chr11
MFG c
P10
P7
Oncogenic rearrangements after the first insertional hit = those
observed in primary T-ALL
All the patients have aditional genetic alterations:
Gain-of function NOTCH1 mutation in P5 and P10
RV induced leukemia = Primary T-ALL ?
Another SCID-X1 gene therapy trial in UK (A. Thrasher)
10 patients median FU 6 Y
Similar MLV-derived RV vector
Good Immune reconstitution
1/10 T ALL at M+24 : LMO2
Gene therapy for SCID-X1 : UK trial
 6
7
8
9
6
7
8
9
1
/
9
100%