E Szerman Les indications et les techniques de préservation de 16

LES INDICATIONS ET LES
TECHNIQUES DE PRÉSERVATION
DE LA FERTILITÉ CHEZ L’HOMME
ET LE JEUNE GARÇON
FORMATION PRESERVATION DE LA FERTILITE EN
CANCEROLOGIE
16 NOVEMBRE 2015

ENVIRON 3000 HOMMES CONGÈLENT
CHAQUE ANNÉE LEURS SPERMATOZOÏDES
DANS LES CECOS AVANT UN TRAITEMENT
GONADOTOXIQUE
PATHOLOGIES CONCERNÉES
PATHOLOGIES CONCERNÉESPATHOLOGIES CONCERNÉES
PATHOLOGIES CONCERNÉES
•CANCERS
•CANCERS TESTICULAIRES (40-50%)
•HODGKIN ET LMNH (15-20%)
•AUTRES HÉMOPATHIES (15-20%)
•AUTRES CANCERS (10%)
•AFFECTIONS NON CANCÉREUSES
(<10%)
•PATHOLOGIE RHUMATOÏDES (TRAITEMENTS PAR
IMMUNOSUPRÉSSEURS)
•INDICATIONS NÉPHROLOGIQUES
•ARTHRODÈSE LOMBAIRE ETC…
•AUTRES INDICATIONS UROLOGIQUES
•TRAUMATISMES, TORSIONS TESTICULAIRES

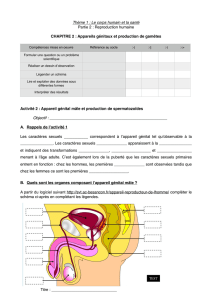
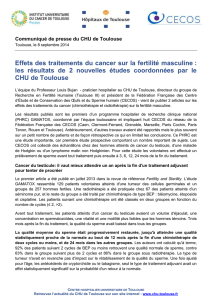
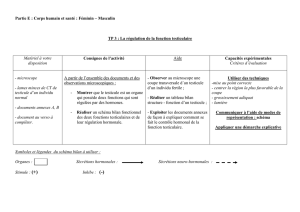
1- Amiens
2- Besançon
3- Bordeaux
4- Caen
5- Clermont-Ferrand
6- Dijon
7- Grenoble
8- Lille
9- Lyon
10- Marseille CHU
11- Montpellier
12- Nancy
13- Nantes
14- Nice
15a- Paris Cochin
15b- Jean Verdier
15c- Paris Tenon
16- Reims
17- Rennes
18- Rouen
19- Strasbourg-Mulhouse
20- Toulouse
21- Tours
Fédération Française des CECOS
réseau de 23 centres
www.cecos.org
1973 – 1er CECOS en France créé
par G. David au Kremlin- Bicêtre

IMPORTANCE DE LA QUALITÉ DE VIE APRÈS
CANCER
•AMÉLIORATION DE LA SURVIE À 5 ANS
•TESTICULE 95%
•HODGKIN 87%
•PLAN CANCER III : SOINS ONCOLOGIQUES DE SUPPORT
•RECOMMANDATIONS ASCO-ASRM-AFSOS –INCA ABM
•LES SURVIVANTS DES CANCERS VEULENT ÊTRE PARENTS ET
ACCORDENT PLUS D’IMPORTANCE AUX LIENS FAMILIAUX.

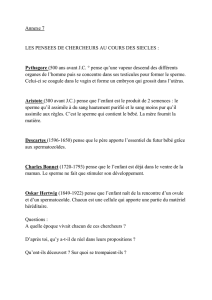
PRISE EN CHARGE EN ONCOFERTILITÉ
Evaluer et repérer
Evaluer et repérerEvaluer et repérer
Evaluer et repérer Informer
InformerInformer
Informer Accompagner
AccompagnerAccompagner
Accompagner
•Les risques de stérilité
secondaire aux
traitements
•Les risques mutagènes
secondaires au traitement
•Le temps disponible pour
planifier une préservation
de la fertilité (avant
démarrage des
traitements
gonadotoxiques)
•Impact des traitements sur
la fertilité (et sur la
sexualité)
•Préservation de la fertilité
: balance bénéfice/risque
•Contraception à prendre
pendant toute la durée du
traitement
•Port du préservatif sous
chimiothérapie (risque de
passage d’agents via le
sperme)
•Brochures et documents
d’information
•Assurer un soutien
psychologique
(consultation possible au
CECOS)
•Dissocier les problèmes
de fertilité des problèmes
de sexualité
•Favoriser la
communication (surtout
chez les enfants et les
adolescents)
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
1
/
27
100%