Gastrointestinal Tuberculosis: Review of Epidemiology & Treatment
Telechargé par
jobeline rajaoarifetra

© 2021 Saudi Journal of Gastroenterology | Published by Wolters Kluwer ‑ Medknow 261
Gastrointestinal tuberculosis: A systematic review of
epidemiology, presentation, diagnosis and treatment
Adnan B. Al‑Zanbagi, M. K. Shariff
Department of Gastroenterology and Hepatology, King Abdullah Medical City, Makkah, Kingdom of Saudi Arabia
Review Article
INTRODUCTION
Tuberculosis, an eighteenth century infectious disease is still
relevant in the twenty‑rst century, despite the emergence
of novel pathogens like coronavirus that is currently
gripping the whole world. Tuberculosis (TB) is signicant
because it infects an estimated quarter of the world’s
population.[1] Though the incidence of TB is the highest
in the Asian and African continents, the developed nations
too are seeing a surge, mainly in latent TB (LTB) due to
immunocompromising diseases, biologic use and migration.
The global burden of TB prompted the United Nations to
forge a declaration by all member states to curb the disease by
2030.[2] Estimated economic impact due to TB is immense;
for example, the annual cost in terms of TB‑related deaths
in a high burden country like India is approximated around
US $30 billion, and to reach its aim, the United Nations
needs an annual budget of US $13 billion.[2,3]
Pulmonary TB is the primary manifestation of tuberculous
infection and is the focus of the World Health Organization
(WHO) strategy to control this disease. However, extra
pulmonary TB is increasing recognized with abdominal
TB being one of the most common presentations as
explained here. Abdominal TB arbitrarily includes infection
of gastrointestinal tract, peritoneum, abdominal solid
organs, and abdominal lymph nodes. Of all the tuberculous
infections of the abdomen, gastrointestinal TB is the most
Tuberculosis (TB) once considered a disease of the developing world is infrequent in the developing world
too. Its worldwide prevalence with a huge impact on the healthcare system both in economic and health
terms has prompted the World Health Organization to make it a top priority infectious disease. Tuberculous
infection of the pulmonary system is the most common form of this disease, however, extrapulmonary TB is
being increasingly recognized and more often seen in immunocompromised situations. Gastrointestinal
TB is a leading extrapulmonary TB manifestation that can defy diagnosis. Overlap of symptoms with other
gastrointestinal diseases and limited accuracy of diagnostic tests demands more awareness of this disease.
Untreated gastrointestinal TB can cause significant morbidity leading to prolonged hospitalization and
surgery. Prompt diagnosis with early initiation of therapy can avoid this. This timely review discusses the
epidemiology, risk factors, pathogenesis, clinical presentation, current diagnostic tools and therapy.
Keywords: Abdominal tuberculosis, clinical features, diagnosis, extrapulmonary tuberculosis, gastrointestinal
tuberculosis, pathogenesis, risk factors, treatment, tuberculosis
Abstract
Address for correspondence: Dr. M. K. Shari, King Abdullah Medical City, PO Box 57657, Makkah Al Mukaramah - 21955, Kingdom of Saudi Arabia.
E-mail: Shari[email protected]
Submied: 14-Mar-2021 Revised: 22-Mar-2021 Accepted: 05-Apr-2021 Published: 30-Jun-2021
Access this article online
Quick Response Code:
Website:
www.saudijgastro.com
DOI:
10.4103/sjg.sjg_148_21
How to cite this article: Al-Zanbagi AB, Shari MK. Gastrointestinal
tuberculosis: A systematic review of epidemiology, presentation, diagnosis
and treatment. Saudi J Gastroenterol 2021;27:261-74.
This is an open access journal, and arcles are distributed under the terms of the
Creave Commons Aribuon-NonCommercial-ShareAlike 4.0 License, which
allows others to remix, tweak, and build upon the work non-commercially, as long
as appropriate credit is given and the new creaons are licensed under the idencal
terms.
For reprints contact: WKHLRPMedknow_reprints@wolterskluwer.com

Al‑Zanbagi and Shari: Gastrointestinal tuberculosis
262 Saudi Journal of Gastroenterology | Volume 27 | Issue 5 | September-October 2021
common site of involvement. The clinical presentation of
gastrointestinal TB is variable to non‑specic making it
challenging to diagnose. This leads to a delay in diagnosis
with consequential serious morbidity. Given its importance
and the need to recognize this old infective foe, we present
a timely review of the epidemiology, pathogenesis, clinical
features, diagnosis and therapy of gastrointestinal TB.
EPIDEMIOLOGY
Despite a steady decline in TB worldwide, around 10
million people were estimated to be ill with it in 2018 of
which more than a million died, making TB the tenth most
common cause of death.[1] TB is primarily an infection of
the lungs (referred to as pulmonary TB), however, it can
affect any organ of the body apart from lungs wherein it
is termed extrapulmonary TB (EXPTB). It was globally
estimated that 8 to 24% of TB cases were extrapulmonary,
making up an average of 15% of the total TB cases notied
to WHO.[1] This variation is reected in the population
and region where the study was carried out. In India, the
country with the highest burden, 20% of TB cases were
EXPTB; of this, 34% were lymphatic TB, 25% pleural,
followed by abdominal at nearly 13%.[4,5] From another
high burden country, China, EXPTB constituted about
31% (6433/20,534) of all TB cases. Of this 31%, the
most common site was, unexpectedly, the skeletal system
(41%; 2643/6433), followed by pleura (26%; 1673/6433).
The abdominal site was not specically looked at, and
the unclassied “other” site formed 14% (873/6433)
of all EXPTB cases.[6] A study from Pakistan, which
carries the fth largest burden of TB, showed that the
proportion of EXPTB was nearly 30% (15790/54092) of
all the notied TB cases; 21% (3313/15790) of EXPTB
cases were abdominal in origin, following pleural (29.6%;
4668/15790) and lymphatic (21.5%; 3581/15790) locations.
[7] In countries with medium‑sized TB burden, EXPTB
constituted 13% (1222/8113) of all TB cases with
9% (105/1222) of these being abdominal TB, making it
the sixth most common site.[8] A low TB incidence country
like the United States had 20% EXPTB (2412/11088)
of all TB cases, with the most common site being the
lymphatics (40%; 1012/2412), and abdomen being the
fourth most common site at 6% (140/2412).[9] Similarly,
in Europe, extrapulmonary location accounted for
17% of all TB cases, with abdomen (3%; 2780/95003)
being the sixth most common site[10] [Table 1]. In South
Africa, a sub‑Saharan country that has high TB and
Human Immunodeciency Virus (HIV) burden, nearly
43% (80/188) of all TB cases presented as EXPTB, and
of this, 28% (22/80) involved the abdomen, the third most
common site after pleura and lymphatics.[11] In a coinfected
population of HIV and TB from a multicenter cohort,
EXPTB accounted for 28% (765/2695) of all TB cases,
with abdominal TB ranking third (11%; 85/765) among
the affected sites.[12]
The incidence of TB in general is dropping across the
globe; however, the proportion of EXPTB is on the rise.
Europe has seen this rise from 16.4 to 22.4% within a
decade,[13] and in the United States, the proportion has risen
from 15.7% in 1993 to 20.4% in 2018. In contrast, the rates
of abdominal TB have remained the same over the years
suggesting that it is following the trends of EXPTB.[9,14]
A rising trend of EXPTB has been reported from a
high‑incidence country like India, too.[15] This rising trend
may in part be due to an increasing awareness and better
diagnostic tools, and additionally may reect an increase
in HIV infections over the years.
RISK FACTORS
Further detailed, studies imply that in general the risk
factors associated with EXPTB tend to be the same as
those for abdominal TB.[10,16,17] In a population‑based study
in the USA that looked at the risk factors for EXPTB, both
EXPTB and abdominal TB were strongly associated with
female gender and end‑stage renal disease.[16] Similarly,
from national TB surveillance data, it was shown that both
EXPTB and abdominal TB were more likely to be related to
young age, female gender, Asian ethnicity and Black race.[17]
A multistate Malaysian study that collected data on EXPTB
from four different states reported similar risk factors for
both EXPTB and abdominal TB. Being female (11% vs
7%), an age of <15 years (20% vs 3%, >65 years), being of
Indian origin (9.4% vs 8% Malaya), having diabetes (9.4%),
being a non‑smoker (7% vs 5%), not consuming
alcohol (9% vs 6%), and being unemployed (9.7% vs 6.4%)
were more likely to have abdominal TB. In comparison,
lymphatic TB, the most common EXPTB site was
more frequently seen in males (28% vs 25%), middle
age group (40% vs 9%), in Malaya (34% vs 27%) and
employed (30% vs 24%) patients without any predilection
for smokers, alcoholics or diabetics.[8] In Europe, having
origins from the Indian subcontinent (adjusted odds
ratio [aOR] = 6.36) or Africa (aOR = 4.64), extremes
of age (<15 and > 64 years) (aOR = 2.21) and female
gender (aOR = 2.02) were strongly associated with
both EXPTB and abdominal TB.[10] A nationwide study
from Pakistan reported similar risk patterns, i.e., female
gender, age <15 years and coming from a specic region
(like a tribal area within Pakistan) for both EXPTB and
abdominal TB.[7]

Al‑Zanbagi and Shari: Gastrointestinal tuberculosis
Saudi Journal of Gastroenterology | Volume 27 | Issue 5 | September-October 2021 263
One of the important forms of TB to consider in risk
factors is LTB. Around 30% of the world’s population
is estimated to be infected with LTB of which 10‑15%
may reactivate to active TB.[18] LTB is more of a concern
in low‑incidence areas of TB such as the United States,
where 80% of active TB cases are due to reactivation of
LTB.[19] Reactivation of LTB tends to present more in the
EXPTB sites, including abdominal TB. England saw a 50%
increase in EXPTB with 80% rise in abdominal TB over a
5‑year period that was mainly attributed to the reactivation
of TB.[20] Hence, factors that increase reactivation of LTB
directly inuence the risk of abdominal TB. Two such
important risk factors are solid organ transplantation and
use of anti‑tumor necrosis factor (TNF) alpha medications.
Immunosuppression
Solid organ transplants (SOT) with immunosuppressants
increase the risk of TB by twenty‑fold, and the proportion
developing EXPTB ranges between 37 and 67%. This
occurs with a corresponding increase in abdominal TB that
is much higher than that of the background population.[21]
In a meta‑analysis of TB in liver‑transplanted patients,
abdominal TB was the most common site accounting for
35% of all EXPTB cases; similarly, in a multicenter study
on TB in renal transplant recipients, abdominal TB was the
leading location, comprising 30% of all EXPTB sites.[22,23]
LTB plays an important role in SOT patients. Untreated
LTB increases the risk of TB with 8.2% developing TB and
none in those treated with a course of isoniazid.[22] TB in
SOT manifests as two peaks following the transplant. The
early peak occurs within the rst 2 years and may be related
to reactivation of LTB and the late peak after 5 years which
is more representative of a new infection.[23] Most TB cases
are diagnosed in the early peak (up to 56%), suggesting
LTB as the main driver for TB in SOT.[23] However, only
around one‑third of transplant patients get screened for
LTB and with an effective therapy to prevent TB infection,
the guidelines recommend active screening for LTB and
treatment of positive cases with 9 months of isoniazid.[24]
Another risk factor is the use of anti‑tumour nectrotic
factor (TNF) alpha medications. TNF alpha is an important
armament in the body’s immune response to TB infection;
decreased activity increases the susceptibility to infection,
and hence, use of anti‑TNF alpha medications is recognized
to reactivate LTB. For this reason, screening for TB prior
to starting this medication is a standard recommendation.
From surveillance data of the food and drug administration
of United States Food and Drug Administration (FDA),
the incidence of TB in patients on anti‑TNF alpha was
fourfold higher than the background rate, and EXPTB
accounted for 56% (39/70) of these TB cases. Abdominal
TB was the third most common form of EXPTB, a higher
than usual proportion, implying an increased association
with anti‑TNF alpha use.[25] This was further conrmed in
a French registry study that reported a similar proportion
of 61% (42/69) of EXPTB with abdominal TB being the
third most common.[26] Though no formal studies on the
risk of TB in developing countries are available, given the
high burden of TB in these regions, the risk associated with
anti‑TNF usage is estimated to be substantially higher, and
thus, EXPTB and abdominal TB are estimated to have a
higher incidence, too.[27]
Co‑infection with HIV
There are more than a quarter of a million deaths due to
TB in HIV‑positive patients worldwide, with 0.8 million
cases of TB linked to HIV infection.[1] HIV‑positive
patients carry a very high risk of developing TB, estimated
to be around twenty‑six‑fold higher than average, and
this risk increases with falling CD4 T cell count. EXPTB,
including abdominal TB, is more common in HIV‑infected
TB patients with low CD4 count.[28] Systemic reviews and
meta‑analysis have suggested that HIV is more commonly
seen in EXPTB than pulmonary TB, more so in patients
with a CD4 count of <100, however, most of the studies
were cross‑sectional in nature.[29,30]
PATHOGENESIS
The mechanism behind EXPTB development is not
fully understood. Various factors involved in the manner
of pathogen interaction with the host may play a role,
however, the dynamics of this is not well‑understood.[28]
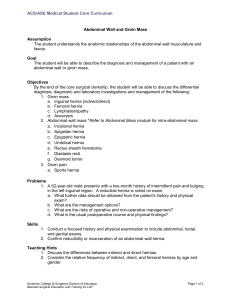
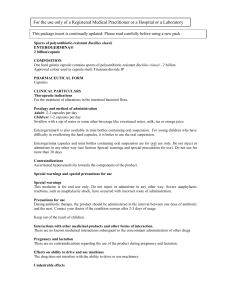
It is now increasingly recognized that the prime route
of transmission of TB is through inhalation that causes
pulmonary infection, followed by the infection of the other
organs by spread from this primary focus [Figure 1]. This
Table 1: Various sites involved in extrapulmonary TB from different countries
Ref. No Country nAbdominal Lymphatics Pleural Bones Nervous system Other sites
4 India 2046 (13 ) (34) (25) (9) (10) (9)
6 China 6433 - 333 (5) 1673 (26) 2643 (41) 440 (7) 873 (14)
7 Pakistan 15790 3313 (21) 3581 (23) 4668 (30) 1483 (9) 725 (5) 2020 (13)
8 Malaysia 1222 105 (9) 324 (27) 227 (19) 116 (9) 122 (10) 328 (27)
9 United States 2 412 140 (6) 1012 (40) 393 (16) 270 (11) 138 (6) 448 (18)
10 Europe 95003 2780 (3) 28019 (29) 38029 (40) 8219 (9) 3180 (3) 14779 (16)
(%) = numbers in parenthesis are percentages; Ref. no=reference number; n=total number of extrapulmonary TB cases

Al‑Zanbagi and Shari: Gastrointestinal tuberculosis
264 Saudi Journal of Gastroenterology | Volume 27 | Issue 5 | September-October 2021
happens predominantly through the lymphatic systems and
the bloodstream. The initial breach from the pulmonary
epithelium to get to the extrapulmonary sites is proposed
to occur by one of these four mechanisms (1) by the help
of macrophages, (2) direct infection of the epithelial
cells, (3) through microfold cells (M cells), a kind of
specialized epithelial cells or (4) by assistance of dentritic
cells.[31] Genetic lineage of TB may determine the EXPTB
site and its clinical presentation with Indian lineage closely
associated with EXPTB.[32] Specic lineages of TB may
have predilection to cause EXPTB due to their ability to
replicate more and invade the macrophages.[33]
Another route of infection postulated is through ingestion
of infected sputum from the lungs [Figure 1]; the ingested
mycobacterium gains entry into the gut through the
intestinal mucosa with the help of M and dendritic cells
as explained previously. Macrophages, mainly present in
the lymphoid tissue in the intestinal mucosa, ingest these
mycobacteria and play an important role in the immune
response. Contagious spread from an adjacent organ is a
possible mechanism that is not entirely explicit.
CLINICAL FEATURES
Abdominal TB encompasses gastrointestinal, peritoneal,
lymph nodal and solid organ involvement; its presentation
is usually chronic or acute‑on‑chronic with non‑specic
symptoms. The duration of illness before diagnosis varies
between weeks and months, some reporting up to 4 years, with
an average of around 8 weeks. The symptoms are insidious
in onset, and include, starting with the most common, fever,
weight loss, night sweats and anorexia. The most frequent
symptoms localized to the abdomen, in descending order of
reporting, are abdominal pain, abdominal distension, nausea/
vomiting, diarrhea and blood in stool. Signs often seen include
abdominal tenderness, ascites, abdominal mass, jaundice,
hepatomegaly and lymphadenopathy.[34‑47]
The most common site of abdominal TB involvement is
the gastrointestinal tract, making 43‑65% of all abdominal
TB cases, followed by peritoneum (20‑47%), lymph
nodes (4‑42%), and then nally solid organs like liver, gall
bladder, spleen and pancreas in 1‑23% of the cases. Up to
33% of the cases have multiple sites and between 15 and
54% have coexistent pulmonary TB [Table 2].[34‑47]
Gastrointestinal tuberculosis
This involves the TB of the upper, middle and the lower
gastrointestinal tract (GIT) from the esophagus to the anus.
Figure 1: Spread of pulmonary TB to abdomen
Table 2: Abdominal TB proportion of different sites
Ref. No nGastrointestinal Peritoneal Lymph nodal Solid organs Mixed Coexist PTB
33 13 9 69 (50) 28 (20) 7 (5) 23 (17) 12 (9)
34 256 127 (50) 106 (41) 10 (4) 7 (3) 58 (23)
35 86 38 (44) 41 (47) 7 (8) 28 (33) 22 (26)
36 17 11 (65) 5 (29) 1 (6)
37 59 26 (52) 16 (32) 8 (16) (54)
38 24 10 (41) 14 (58) 3 (12) 10 ( 41)
39 58 25 (43) 27 (47) 18 (31) 2 (8) 10 (17)
40 57 33 (58) 13 (23) 24 (42) 11 (20) 27 (47)
41 93 51 (51) 33 (33) 41 (41) 27 (29)
42 31 15 (48) 11 (35) 5 (17) 11 (35)
43 46 7 (15)
44 40 (60) (40)
45 65 23 (35) 2 (3) 22 (33) 20 (31)
46 209 103 (49) 87 (42) 9 (4) 10 (5) 134 (64)
Total 118 0 43-65% 20-47% 4-58% 1-20% 9-33% 3-64%
() = numbers in parenthesis are percentages; Ref. no=reference number; n=total number of abdominal TB cases; Solid organs include liver, spleen
and/or pancreas; PTB=pulmonary tuberculosis

Al‑Zanbagi and Shari: Gastrointestinal tuberculosis
Saudi Journal of Gastroenterology | Volume 27 | Issue 5 | September-October 2021 265
Pathogenesis of gastrointestinal tuberculosis
Gastrointestinal tuberculosis (GITB) infection follows
the same pattern described previously for abdominal
TB, which includes hematogenous, lymphatic, direct and
ingestion route of spread. In addition, ingestion of milk or
food infected with bovine mycobacterium was previously
a well‑recognized route, however, the pasteurization of
milk and prevention of bovine mycobacterial infection in
livestock has made this rare. Whether GITB occurs as a
primary infection, or as a secondary spread from pulmonary
focus, is not well‑dened; coexisting pulmonary TB and
GITB is reported in 13‑67% of the cases, with some
arguing that this probably is an underestimate, due to
unrecognized or asymptomatic primary focus.[48‑54]
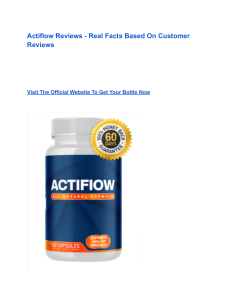
Once the mycobacterium invades into the submucosa
through the mucosa of the intestine, it initiates a
granulomatous inammatory response including vasculitis
with thickening of the submucosa and serosa; this leads to
ulceration that can perforate or heal by brosis. Pathological
intestinal TB can manifest as ulcerative, hypertrophic,
ulcero‑hypertrophic or in brotic forms. Complications
occur as a result of these different forms of enteritis and
present as strictures causing obstruction or perforations,
including stulas [Figure 2]. Rarely, hemorrhagic enteritis
can occur.[49,55,56]
Clinical presentation of gastrointestinal tuberculosis
TB can involve any site of the GIT from the esophagus
to the anus, including the perianal region. However, it
has a predilection for the ileocecal region, which is the
most commonly infected site accounting for 44‑84% of
all GITB cases.[34‑42,50‑53] The physiology and anatomic
pathology of a constricted ileocecal region, which leads
to long contact time, increased absorption and abundant
lymphatic tissue, explains the predisposition.[48,49] The
other common sites of involvement include caecum,
ileum, ascending colon, transverse colon, descending
colon, jejunum and rectum.[34‑42,50‑53] It rarely infects the
upper GIT (esophagus, stomach, duodenum) and anus
[Table 3].[34‑36,39,41,52,53]
Gastrointestinal TB of the twenty‑rst century is a disease
of the young, with a mean age ranging between 32 and
Figure 2: Mycobacterium invades the submucosa leading to formation of granulomas, vasculitis and hypertrophy, which in turn cause ulcers,
perforation, stulas and abscess formation
Table 3: Gastrointestinal TB proportion of different infected sites
Ref. No nIleocecal Large bowel Esophagus Stomach Duodenum Small bowel
33 69 46 (67) 12 (17) 3 (4) 3 (4)
34 212 122 (58) 6 (3)
35 38 14 (37) 6 (16) 2 (5) 2 (5) 4 (36)
36 11 5 (45) 2 (18)
37 26 20 (40) 6 (12)
38 8 3 (38) 3 (38) 1 (1)
39 25 14 (56) 5 (20) 2 (8) 1 (4) 1 (4) 2 (8)
40 33 2 (6) 28 (85)
41 51 16 (31) 36 (71)
49 85 56 (66)
50 81 46 (84)
51 61 26 (44) 16 (26) 21 (34)
52 104 29 (28) 6 (6)
Total 719 44%-84% 3%-71% 4%-8% 4%-6% 1%-6% 8%-85%
Ref. no=reference number; () = numbers in parenthesis are percentages; n=total number of gastrointestinal TB cases
 6
7
8
9
10
11
12
13
14
6
7
8
9
10
11
12
13
14
1
/
14
100%