CLINICAL ORTHOPAEDICS AND RELATED RESEARCH
Number
339,
pp
82-91
0
1997
Lippincolt-Raven
Publishers
Modified Transverse Locking Nail
Fixation
of
Proximal Femoral Fractures
B.H.
Ziran, MD;
N.A.
Sharkey, PhD;
T.S.
Smith,
MS;
G.
Wang;
and
M.
W. Chapman, MD
It
was hypothesized that transverse locking
screws of intramedullary nails, seated above
the lesser trochanter, provide equal strength to
that of reconstruction nails, and that screws
placed through the medial cortex of the
femoral neck do not have adverse biomechani-
cal effects during physiologic loading. Syn-
thetic femurs (n
=
10)
and paired anatomic
specimen femurs (n
=
14)
were tested intact
and with an intramedullary device in place. In-
tact specimens were loaded nondestructively,
then a segmental subtrochanteric defect was
created and either a high seated transverse
locking nail or a reconstruction nail was in-
serted and statistically locked. Axial and tor-
sional stiffness were determined followed by
axial failure testing. Mechanical parameters
evaluated were stiffness, displacement, and en-
ergy. The implanted specimens did not show
any statistically significant difference between
transverse
or
reconstruction screw constructs
with any of the measured parameters (stiff-
ness, displacement, and energy). Failure tests
in implanted specimens also did not show any
statistically significant difference in yield load,
yield displacement,
or
energy to failure be-
From the Department of Orthopedic Surgery, Univer-
sity of California, Davis, Sacramento. CA.
Implants were provided by Howmedica Inc, Ruther-
ford,
NJ.
Reprint requests
to
B.H.
Ziran,
MD,
Department
of
Or-
thopedic Surgery, University
of
Pittsburgh,
1010
Kauf-
man Building,
3471
Fifth Avenue, Pittsburgh,
PA
15213-3221.
tween implant constructs. All anatomic speci-
mens failed, with fractures
of
the proximal
fragment involving medial and lateral cortices.
Synthetic specimens did not fracture but
showed failure with implant deformation at
the level of the skeletal defect. The use of high
seated transverse locking nails for complex
proximal femoral fractures is a viable option
and has comparable in vitro mechanical per-
formance with reconstruction nails. Although
not shown to be
a
problem in the present study,
clinical evaluation of screws through the me-
dial femoral neck cortex is required.
Fixation of unstable fractures of the proxi-
mal femur particularly is challenging be-
cause of the large axial forces and bending
moments occurring in this regi0n.6JlJ5~14~26
Although standard intramedullary nails offer
distinct advantages to plates, in cases where
the posteromedial buttress
is
not intact, nails
where the proximal interlocking mechanism
uses screws directed
up
the femoral neck
into the femoral head (hereby referred to as
reconstruction nails) or plates must be
used.24.7.
16,18325
One of the commercially
available transverse locking nails (Alta
femoral nail, Howmedica, Rutherford, NJ)
potentially is useful for such fractures be-
cause of the design of the proximal fixation.
The proximal holes for crosslocking screws
in this nail are closer to the top of the nail
than other nail designs, and therefore can be
82

Number 339
June, 1997 Modified Transverse Locking Nail Fixation
83
placed
above
the
lesser
trochanter, achieving
fixation
in
the
femoral
neck
or
the
femoral
head.
The
purpose
of this
study
was
to
measure
the
acute
strength
of
a
fixation
construct
in
a
simulated unstable
proximal
femoral fracture,
comparing intramedullary
nails
locked
with
transverse
screws
to
those locked with recon-
struction screws.
MATERIALS AND METHODS
Experimental Design
In the first experiment, synthetic femurs (Saw-
bones, Pacific Labs, Seattle
WA)
were tested non-
destructively in torsion and axial loading. The
specimens were first tested intact, and then after
fixation of a simulated unstable proximal femoral
fracture. The independent variable of interest was
fixation device (nails using transverse screws
or
reconstruction screws for proximal fixation); the
dependent variables measured were stiffness, de-
formation, energy to peak load, and energy
loss
in
cyclic loading.
In the second experiment, the synthetic femurs
from the first experiment, and
as
paired human
anatomic specimen femurs with simulated unstable
proximal fracture, stabilized with either transverse or
reconstruction screw fixation, were loaded to failure
in axial compression. The independent variables of
interest were specimen type (synthetic, fresh, or em-
balmed bone) and fixation method (transverse screws
or reconstruction screws), and the dependent vari-
ables were stiffness, yield displacement, yield load,
yield energy, and mode of failure.
Specimens
The synthetic bones (n
=
14) tested were second
generation composite bones,
42
cm in length,
consisting of a resin covered fiberglass cortex
and a plastic foam filled medullary canal. The
stiffness of these bones is close to that of fresh
human femurs, and the specimen to specimen
variation is much less (coefficient of variation
<7.3%). However, the composite bones are con-
siderably more elastic than fresh human bones,
with only approximately
1/5
the energy
loss
per
loading cycle in axial compressive loading2L.22
(nonpublished data, Ziran
BH,
Sharkey
NA,
Smith TS, Wang
G,
Chapman
MW
Comparisons
between synthetic and cadaveric bone specimens
in biomechanical testing 1995).
The human anatomic specimen bones used
in
the second part of the study included two pairs
of
fresh femurs and five pairs of embalmed femurs.
Age of the donors was unknown. All human spec-
imens were radiographed before testing to rule
out any obvious pathology. In addition, the speci-
mens underwent computed tomography
(CT)
scanning at various levels to measure density and
describe morphology. Density was recorded from
two levels (cephalad and central) in the femoral
head, from two intracortical loci
on
the lateral
cortex of the femoral neck, and from one intracor-
tical locus on the medial cortex of the femoral
neck. Morphologic measurements included
femoral neck diameter at the subcapital level, in-
ner and outer cortical diameters at the sub-
trochanteric level, offset
of
the femoral head from
the medullary canal, and total cross sectional area
at the head, neck, and subtrochanteric levels.
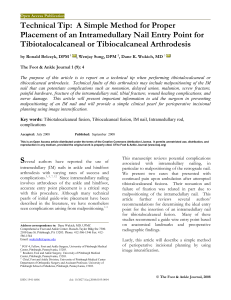
Specimen Preparation
Distally, femurs were potted in polymethyl-
methacrylate to the level of the epicondyles, with
several embedded screws to prevent rotation.
Proximally, the caudad
1/2
of the femoral head
was similarly embedded in polymethylmethacry-
late in a fashion that allowed loading through the
femoral head (Fig
1).
The anatomic specimen fe-
murs were stripped of all soft tissues and the dis-
tal femoral condyles were removed parallel to the
transverse plane. At this point, mounting
in
poly-
methylmethacrylate was done identically to the
synthetic femurs.
After mechanical testing of the intact bones
(synthetic and anatomic specimen), an unstable
proximal femoral fracture was simulated by re-
moving a 3-cm segment of bone. Transverse saw
cuts were made at 1 and
4
cm below the lesser
trochanter, and the intercalary segment was re-
moved. The lesser trochanter also was removed,
but the lateral cortex at this level was left intact to
allow lateral cortical purchase for both types of
fixation screws (Fig
1).
In the synthetic specimens, canals were
reamed to 14-mm diameter for implantation of
a 13-mm
x
380-mm nail. In the human
anatomic specimens, canals were reamed
1
mm larger than the size at which the reamer
began cutting the inner endosteal cortex (chat-
ter). With this technique, anatomic specimens
all received 13-mm nails whose lengths were
variable depending on the length of the specimen.

Clinical
Orthopaedics
84
Ziran
et
al
arid
Related Research
by the same trauma surgeon
(BHZ)
who had clini-
cal experience using both fixation systems.
Mechanical Testing
Fig
1.
Osteotomized femur in loading appara-
tus for axial testing. Note transverse screws
placed cephalad to lesser trochanteric level.
In specimens fixed with reconstruction screws,
the upper fragment was reamed to
17
mm diame-
ter to accommodate the larger proximal segment
of the nail.
Transverse locking screws were placed
so
that
the most proximal screw exited the medial fe-
moral cortex in the subcapital area and the more
distal of the proximal screws exited above the
lesser trochanter (Fig 1). The reconstruction
screws were placed into the femoral neck and head
without penetration
of
the femoral head. Distally,
all nails were statically locked with two screws.
Reaming and nailing were done in the laboratory
Axial testing was done using an Instron 1122
testing machine (Instron Corp, Canton, MA)
equipped with a
5-kN
axial load cell. The testing
device was interfaced to a personal computer us-
ing Asyst scientific software (Asyst Software
Technologies, Inc, Rochester,
NY)
and an analog
to digital measurement and control system (Series
500,
Keithley Instruments, Inc, Cleveland,
OH).
Specimens were mounted on a turnstile and
loaded along the mechanical axis, with the
femoral head centered over the condyles. Simu-
lation of muscle loading was not done.13 For non-
destructive testing, specimens were loaded
cyclically in compression at 10 mm per minute
top peak loads
of
1000
N,
and loads were
recorded at 0.05-mm increments of displacement.
Each femur was subjected to five conditioning
loads followed by five loading cycles from which
data were collected and averaged. Destructive
ax-
ial testing was done with a ramp load to failure
after several low conditioning cycles to
500
N.
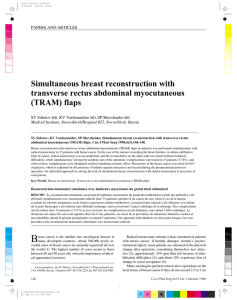
During testing in torsional loading (synthetic
specimens only), the femoral head was mounted
by means of an adjustable fixture to a 250-Nm
torsional load cell. The base of the femur was
mounted to an xy sliding table. The fixture was
adjusted
so
that the axis of rotation was collinear
to the axis of the femoral nail (Fig 2). A torsional
stepper motor (Model
S83-93,
Compumotor,
Rohnert Park, CA) in series with the load cell was
mounted to the Instron crosshead. The specimens
were loaded cyclically at a rate
of
0.05
rad per
second up to 10 Nm of torque. Loading was alter-
nately clockwise and anticlockwise from the neu-
tral position. After five conditioning cycles, data
were collected and averaged from five loading
cycles (Fig 2).
Analysis
of
Findings
The structural stiffness in the nondestructive tests
was calculated as the slope of the last six digi-
tized data points before achieving peak load and
using elastic portion of the load displacement
curve for destructive tests. Energy to peak load
was calculated as the area under the load versus
displacement curve. Energy loss per cycle was
the percentage difference in area under the load-
ing and unloading load versus displacement

Number
339
June,
1997
Modified Transverse Locking Nail Fixation
85
Fig
2.
Osteotomized specimen mounted
for
torsional testing. Base mounted on an x
y
table
to allow centering and to reduce extraneous
loading.
curves. The
95%
secant method
was
used to de-
termine yield load in destructive
tests
(the inter-
section
of
the
load
versus
displacement
curve
with
a
line
whose
slope
is
95%
of
the
elastic por-
tion
of the
load
versus
displacement
curve).
A
nonpaired test was
used
for
the
nondestruc-
tive
tests
using the synthetic
femurs.
For
the
de-
structive axial tests,
a
two-way analysis
of
variance
(ANOVA)
comparing specimen type syn-
thetic, fresh anatomic specimen, embalmed
anatomic specimen) and fixation
method
(trans-
verse screws or reconstruction screws)
was
done,
using
a
Tukey followup test. Side
to
side differ-
ences in
the
anatomic specimen groups were
ana-
lyzed using
a
paired
t
test.
The
effects
of
bone den-
sity
and
morphologic variable measured from
the
CT
scans
in relation to mechanical properties were
evaluated using
a
stepwise
linear
regression.
RESULTS
In the nondestructive axial loading tests, there
were no significant differences in stiffness,
displacement, energy to peak load, or energy
loss between constructs stabilized with trans-
verse screw or reconstruction screw methods.
However, both of these constructs were con-
siderably less stiff and less elastic (greater en-
ergy loss) than the intact synthetic femurs (Fig
3).
Similarly, in torsional testing the two con-
structs had very similar mechanical values, but
both were
30%
to
40%
as stiff and less elastic
than
the
intact femurs (Table
1,
Fig
4).
In the axial tests to failure,
ANOVA
indi-
cated that there was a significant effect of spec-
imen type (synthetic bone versus anatomic
specimen bone) for yield displacement (p
<
0.02)
and stiffness (p
<
0.01).
There were no
statistically significant differences in any para-
meter between fixation devices (transverse
screw or reconstruction screw) in the anatomic
bone specimens or the synthetic bone speci-
mens (Table
2,
Figs.
56).
Gross examination of the failed speci-
mens revealed several differences in failure
mechanism between specimen types and fixa-
tion devices. In the synthetic specimens, trans-
verse screw specimen constructs failed by
bending of the nail at the more distal of the two
proximal screw holes (Fig
7);
frequently the
screw in this hole bent as well. In synthetic
specimens with reconstruction screw fixation,
failure occurred by bending of the nail at the
level where it increases diameter proximally
(Fig
8).
The most proximal screw often bent,
but did not cut out. There were no femoral neck
fractures in the synthetic specimens.
In human anatomic specimen bone, failure
occurred by a combination of bone failure and
bending of the fixation device. Typically, bone
failure would initiate at a screw hole and
progress to a basicervical fracture of the
femoral neck. In transverse screws constructs,

Clinical Orthopaedics
86
Ziran
et
al
and Related Research
TABLE
1.
Axial and Torsional Nondestructive Testing Data
Test
Intact Screws (n
=
7)
Screws (n
=
7)
Reconstruction Transverse
Axial (n
=
14)
Stiffness (N/mm)
1369
*
100 533
+.
70 532
~t
39
Energy
to
peak load (N-m)
0.38
*
.03 1.04
*
0.15 1.05
*
0.12
Axial displacement (rnm)
0.8
*
0.1 2.3
*
0.4 2.4
i
0.4
Energy loss
(%)
1.7 14.2 15.1
Stiffness (N/rnm)
323
*
22 108
+
10 126
i
23
Energy
to
peak load
(N-rn)
0.17
*
.01 0.50
&
.02 0.46
*
.05
Torsional
(n
=
14)
Displacement
(")
2.2
*
.01 5.4
*
2.0 4.4
*
1.9
Energy
loss
(%)
8.3 20.4 20.1
There
were
no
statistically significant differences
between
implant
types
the fracture started in the medial cortex of the
femoral neck at the site of the more caudad
proximal interlocking screws (Fig
9).
In re-
construction screw constructs, the fracture
started on the lateral side at the site of the more
caudad locking screw, but ultimate failure in-
volved the medial cortex of the neck (Fig
10).
In all cases, progression to failure occurred
with bending
of
the implant and fracture of the
femoral neck.
No
differences were observed
between fresh and embalmed specimens and
no side
to
side differences in failure were seen.
Computed tomographic data
of
the intact
anatomic specimen bones were used
to
pro-
TABLE
2.
Axial Test to Failure
vide geometric and densitometric inputs for
a stepwise linear regression analysis.
No
as-
sociations were found between the geometric
or densitometric data and the mechanical be-
havior
of
the construct under axial load. Side
to side variances and subject to subject vari-
ances were not statistically significant.
DISCUSSION
The authors found no differences in the me-
chanical properties of unstable proximal
femoral fractures fixed with either transverse
or reconstruction locked intramedullary nails.
Test Reconstruction Transverse
Screws (n
=
7)
Screws (n
=
7)
Anatomic specimen bones (n
=
Stiffness (N/mm)*
Yield load
(N)
Yield displacement (mm)**
Yield energy (N-m)
Synthetic bones
(n
=
14)
Stiffness (N/mm)*
Yield load (N)
Yield displacement (mm)**
Yield energy
(N-rn)
14) 163
*
44
2705
*
813
19+7
32
5
21
533
*
70
3165
f
930
13
*
4
22
*
11
149
+
57
2763
f
558
23
+
10
36
*
20
532
*
39
2672
*
796
12+5
17
+
10
*p
<
0
01
**D < 0.02
 6
7
8
9
10
6
7
8
9
10
1
/
10
100%