วารสาร
เทคนิคการแพทย์และกายภาพบำาบัด
JOURNAL OF MEDICAL TECHNOLOGY AND PHYSICAL THERAPY
นิพนธ์ต้นฉบับ
ORIGINAL ARTICLE
J Med Tech Phy Ther Vol. 30 No. 3 September - December 2018
อิทธิพลการคลาย sacrotuberous ligament ด้วยการทดสอบ Faber
ในคนสุขภาพดี
1 1*1
Received: February 11, 2018
Revised: June 3, 2018
Accepted: June 11, 2018
บทคัดย่อ
วัตถุประสงค๋:
วิธีการ :
ผลการด�าเนินการ :
p
สรุป :
ค�าย่อ :
ค�าส�าคัญ:
1

วารสาร
เทคนิคการแพทย์และกายภาพบำาบัด
JOURNAL OF MEDICAL TECHNOLOGY AND PHYSICAL THERAPY
นิพนธ์ต้นฉบับ
ORIGINAL ARTICLE
Inuence of releasing sacrotuberous ligament to Faber test
in healthy individuals
111
Received: February 6, 2018
Revised: May 14, 2018
Accepted: Jun 4, 2018
Abstract
Objectives:
Method :
Results :
Conclusion :
Abbreviation :
Keywords:

J Med Tech Phy Ther Vol. 30 No. 3 September - December 2018
Introduction
(1)
(2)
(3)
(6)
(3)
(7)
(1)
1 (7)
(9)
(11)

Material and Methods:
Participants
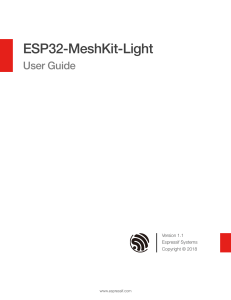
Instrumentation :
Figure 1
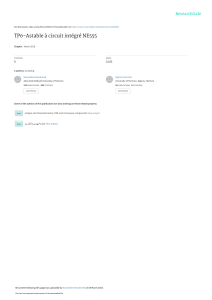
Procedure :
Figure 2)
Figure 2
B
A

J Med Tech Phy Ther Vol. 30 No. 3 September - December 2018
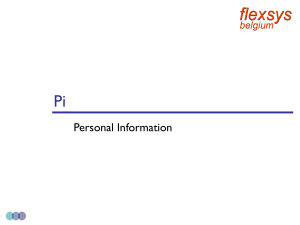
Figure 3)
Figure 3
Figure 4)
Figure 4
Data analysis
Results
Table 1
Table 1
Characteristics Mean + SD
2)
 6
7
8
6
7
8
1
/
8
100%