Chapter 119
Aseptic meningitis
LISE E. NIGROVIC*
Department of Medicine, Children’s Hospital Boston and Harvard Medical School, Boston, MA, USA
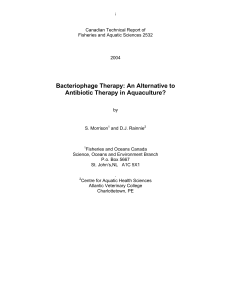
Meningitis refers to inflammation of the cerebrospinal
fluid (CSF) and the meninges that surround the brain
and spinal cord (Fig.119.1). Aseptic meningitis or viral
meningitis cases occur at any age but are most common
in infants and young children. Most cases of aseptic
meningitis have a benign, self-limited course with
maximal symptom duration of 1–2 weeks. The youngest
patients, particularly neonates within the first few weeks
of life, typically have the most severe symptoms. Menin-
goencephalitis occurs when infection involves the brain
parenchyma as well as the meninges.
CLINICAL PRESENTATION
Young children and infants with meningitis may present
with nonspecific signs: fever, irritability, lethargy, poor
feeding, or vomiting (Rittichier et al., 2005). Older chil-
dren with meningitis may present with fever, photopho-
bia, headache, or stiff neck. Seizures are most common
with herpes meningoencephalitis. Physical examination
findings such as the Brudzinski sign (active flexion of
the neck results in passive flexion of the patient’s hip)
and Kernig sign (pain with knee extension when the
hip is flexed), although rare, are highly suggestive of
meningitis.
DIAGNOSIS OF MENINGITIS
A lumbar puncture is diagnostic of meningitis and should
be performed as soon as the patient’s clinical stability
allows. Head computed tomography prior to lumbar
puncture need not be performed routinely, but should
be considered when the child has evidence of increased
intracranial pressure or a fucal neurologic exon because
of the risk of subsequent cerebral herniation. Signs of
increased intracranial pressure include a bulging fontanel,
blurred optic disk margins, or any focal neurological
deficit. Antibiotic pretreatment prior to diagnostic evalu-
ation for possible meningitis should lower the clinical
threshold to perform a diagnostic lumbar puncture due
to the potential of partially treated bacterial meningitis.
A case of aseptic meningitis is defined by the presence
of CSF pleocytosis (CSF white blood cell (WBC) 10
cells/mm
3
) with a negative CSF bacterial culture in a
patient who has not received prior antibiotics. Bleeding
due to traumatic insertion of the lumbar puncture needle
complicates the interpretation of the CSF analysis due to
the introduction of both red blood cells (RBCs) and
WBCs. Although several methods of correcting CSF
WBCs for the presence of RBCs have been developed,
none of these methods can accurately identify all cases
of meningitis (Bonadio et al., 1990). Use of local anes-
thetic and removal of the catheter stylet after the lumbar
puncture needle pierces the skin are modifiable proce-
dural factors that have been shown to reduce the rate
of traumatic lumbar puncture (Nigrovic et al., 2007b).
MICROBIOLOGY
In the era of widespread vaccinations against bacterial
pathogens, most cases of meningitis are caused by viral
not bacterial infection. Enteroviruses are picornaviruses
which are responsible for the vast majority of aseptic
meningitis cases (85–95% of cases in which a pathogen
is identified; Lee et al., 2006). The picornavirus family
includes echovirus, Coxsackie A and B viruses, as well
as the polioviruses. Poliovirus, although exceedingly rare
due to effective widespread vaccination, results in selec-
tive destruction of the motor neurons leading to flaccid
paralysis. Enterovirus 71 has been linked to several
recent outbreaks of encephalitis with high associated
mortality. Although these infections occur year round,
peak yearly incidence in temperate climates occurs
*Correspondence to: Lise E. Nigrovic, M.D., M.P.H., Assistant Professor of Pediatrics, Department of Medicine, Children’s
Hospital Boston and Harvard Medical School, 300 Longwood Avenue, Boston, MA 02115, USA. Tel: þ1-617-355-6363,
Fax: þ1-617-730-0335, E-mail: [email protected]
Handbook of Clinical Neurology, Vol. 112 (3rd series)
Pediatric Neurology Part II
O. Dulac, M. Lassonde, and H.B. Sarnat, Editors
©2013 Elsevier B.V. All rights reserved

during the summer and fall months (June through
October). Transmission of the enteroviruses occurs via
the fecal–oral route, although inhalation of infected
droplets has also been reported. The incubation period
is usually 3–6 days.
Other less common viral causes include the following:
Epstein–Barr virus, herpes simplex, human paraecho-
virus, mumps, and varicella-zoster virus. Aseptic menin-
gitis may also be caused by nonviral infections
(Bartonella henselae (cat scratch disease), Borrelia
burgdorferi (Lyme disease), Cryptococcus,Mycobacte-
rium tuberculosis (Mollaret’s meningitis), Rickettsia
species, Mycoplasma pneumoniae) or noninfectious
entities (drugs, autoimmune/collagen vascular diseases,
Kawasaki disease).
DISTINGUISHING ASEPTIC FROM
BACTERIAL MENINGITIS
Definitive discrimination between aseptic and bacterial
meningitis depends on the results of the CSF culture;
it takes 2–3 days to exclude bacterial growth reliably.
Meningeal signs (defined by the presence of neck stiff-
ness, Kernig’s or Brudinski’s sign, or bulging fontanelle
in an infant) are associated with the presence of bacterial
meningitis but also aseptic meningitis, pneumonia, deep
neck-space infections, as well as other self-limiting dis-
eases such as myalgias or torticollis.
Clinicians use CSF results to distinguish bacterial
from aseptic meningitis. CSF Gram stain is the best
single predictor with a sensitivity of approximately
65% depending on the bacterial pathogen and the colony
count. Other CSF parameters such as WBC count, glu-
cose, or protein have a wide zone of overlap between
bacterial and aseptic meningitis. Biomarkers such as
C-reactive protein or CSF lactate may not show elevation
early in bacterial disease and may also be elevated in
patients with viral infections. Recent studies suggest that
procalcitonin (which is in widespread clinical usage in
Europe but not the USA) may have a role in discriminating
between aseptic and bacterial meningitis, although further
investigations are needed (Dubos et al., 2006a). Enterovi-
ral polymerase chain reaction (EV-PCR), however,
provides a means to identify positively cases of viral men-
ingitis. A new commercially available PCR testing plat-
form can provide clinicians with EV-PCR results within
a few hours, having the potential to affect management
decisions about antibiotic administration and disposition
(Ramers et al., 2000; Archimbaud et al., 2009).
Multivariate clinical prediction rules combine readily
available clinical and laboratory parameters to distin-
guish cases of bacterial from aseptic meningitis. One
meningitis prediction rule (the Bacterial Meningitis
Score) was validated on a large multicenter cohort in
the era of widespread conjugate pneumococcal vaccina-
tion. This prediction rule identifies a group of patients at
very low risk of bacterial meningitis if they lack all of the
high-risk criteria (Table 119.1;Nigrovic et al., 2002,
2007a) and has now been validated in eight published
studies (Nigrovic et al., 2012). Application of a validated
meningitis decision rule has the potential to help clini-
cians improve the care of children with CSF pleocytosis
Fig.119.1. Cross-sectional anatomy. Meningitis is caused by inflammation of cerebrospinal fluid (CSF) and the meninges that
surround the brain and spinal cord. Reprinted with permission from Torpy et al., 2007. Copyright 2007 American Medical
Association.
1154 L.E. NIGROVIC

by identifying a subset of patients at very low risk of bac-
terial meningitis who could, in the appropriate clinical
context, be managed as outpatients after strong consid-
eration of administration of a long-acting parenteral
antibiotic (Dubos et al., 2006b, 2008). Meningitis clinical
prediction rules should be applied cautiously to the youn-
gest infants (2 months of age), who are most likely to
be misclassified and who are the most difficult to eval-
uate clinically. Clinicians also need to be aware that these
prediction models do not identify patients at risk of other
treatable types of central nervous system infections such
as Lyme meningitis or herpes encephalitis.
PRETREATED MENINGITIS
Administration of antibiotics prior to lumbar puncture
may render CSF culture results falsely negative, making
the determination of the appropriate duration of antibi-
otics more difficult (Kanegaye et al., 2001). When bacte-
rial meningitis is clinically suspected, however, empirical
antibiotics should be started without delay even if
the diagnostic lumbar puncture is to be deferred. Antibi-
otic pretreatment has also been shown to affect CSF
profiles by decreasing CSF protein and increasing CSF
glucose without significant effects on CSF cell counts
(Nigrovic et al., 2008). Therefore, clinical prediction
rules for bacterial meningitis should not be applied to
patients pretreated with antibiotics. CSF latex agglutina-
tion tests detect the presence of bacterial antigens in the
CSF but have low sensitivity and limited clinical utility.
TREATMENT
Viral meningitis is treated with supportive measures
alone. Inpatient care is required only for intravenous
hydration and pain control. No currently available anti-
viral agents have activity against enteroviruses. Defini-
tive exclusion of bacterial infections depends on
bacterial culture results, which take several days to reli-
ably exclude bacterial growth. Empirical antibiotics
should be initiated early for all patients with a clinical
concern for bacterial meningitis. For these patients, anti-
biotics should be selected to have a broad antimicrobial
spectrum that covers the likely bacterial pathogens and
known resistance patterns. The duration of antibiotics
should be determined by a combination of clinical pre-
sentation, viral diagnostics, and bacterial culture results.
MENINGOENCEPHALITIS
Children with meningoencephalitis present with acute
onset of altered mental status, focal neurological defi-
cits, ataxia, aphasia, or focal seizures. Most children will
also have an associated fever. Examination of the CSF
typically reveals a mild pleocytosis with a lymphocytic
predominance.
Herpes simplex virus (HSV) is the most commonly
identified cause of encephalitis and occurs in patients
of all ages. Neonates are particularly susceptible to
HSV infection, with most cases transmitted peripartum
(although in utero and postnatal transmission are also
reported). Neonatal HSV meningitis often occurs without
cutaneous findings and typically presents within the first 2
weeks of life. If HSV infection is suspected, CSF should
be obtained for PCR detection as well as routine studies.
Abnormalities in the temporal lobe region on neuroimag-
ing suggest HSV encephalitis, although the viral tropism is
not specific enough to enable definite identification of the
infecting virus. Aciclovir therapy should be initiated pend-
ing diagnostic test results. Children with proven HSV
encephalitis should be treated with intravenous aciclovir
for 21 days as well as long-term suppressive therapy
(Kimberlin et al., 2011). Even after appropriate diagnosis
and treatment, children with HSV encephalitis can have
significant associated morbidity and mortality.
Arthropod-borne viruses cause epidemic encephali-
tis. Because the mosquito is the most common vector,
most cases occur during the summer months when insect
activity is the highest. West Nile encephalitis was first
reported in the West Nile district of Uganda in the
1930s. Now, West Nile virus has been detected in 46
of the states (concentrated in the East and South) as
well as throughout Europe. Other causes of arborviral
encephalitis in the USA include: eastern equine,
La Crosse, St. Louis, and western equine viruses. Ther-
apy for arborvirus infection is largely supportive,
although empirical acyclovir should be considered until
HSV infection can be definitely excluded. Most patients
make a complete recovery, although some patients with
arborviral encephalitis are left with seizure disorder or
persistent neurological deficits.
Influenza virus infection (particularly type A)
has also been rarely associated with encephalitis. The
incidence of neurological complications is highest in
children under 5 years of age. Viral transmission occurs
person to person through respiratory secretions with a
peak incidence during the winter months (January
through February).
Table 119.1
Bacterial Meningitis Score: five high-risk criteria
Positive CSF Gram stain
CSF absolute neutrophil count (ANC) 1000 cells/mm
3
CSF protein 80 mg/dL
Peripheral blood ANC 10 000 cells/mm
3
Presence of a seizure at or prior to presentation
From Nigrovic et al. (2007a).
ASEPTIC MENINGITIS 1155

NONINFECTIOUS CAUSES
Aseptic meningitis can result from noninfectious causes
such as medications. Drugs that have been implicated as
possible causes of aseptic meningitis include nonsteroi-
dal anti-inflammatory drugs (NSAIDs), sulfa drugs, and
intravenous immunoglobulin (IVIG). Medication-
induced aseptic meningitis must remain a diagnosis of
exclusion after other more common infectious causes
have been effectively excluded.
RECURRENT ASEPTIC MENINGITIS
Recurrent or Mollaret meningitis is an extremely rare
clinical entity defined as three or more episodes of asep-
tic meningitis. Patients present with fever and meningis-
mus lasting several days followed by spontaneous
resolution. There is considerable patient-to-patient vari-
ability in the time between episodes (weeks to years). The
CSF reveals a mild pleocytosis with a lymphocytic pre-
dominance. Most commonly, these episodes are caused
by HSV (type 1 or 2) infection identified by PCR testing
of the CSF. Patients often do not have a history of genital
lesions. Noninfectious causes of Mollaret meningitis,
such as an epidermoid cyst, must also be considered.
CONCLUSIONS
Aseptic meningitis is a common but typically benign child-
hood infection. The incidence is highest in infants and dur-
ing the summer months. Affected children typically make a
complete recovery with supportive care alone. Because of
the overlap between the clinical and laboratory features of
patients with aseptic and bacterial meningitis, many
patients with aseptic meningitis are treated with empirical
antibiotics while awaiting bacterial culture results. Viral
diagnostics allow for more rapid exclusion of bacterial
infection as well as initiation of specific therapy when avail-
able. Meningoencephalitis may cause more severe neuro-
logical symptoms, but clinical care is largely supportive.
REFERENCES
Archimbaud C, Chambon M, Bailly JL et al. (2009). Impact of
rapid enterovirus molecular diagnosis on the management
of infants, children, and adults with aseptic meningitis.
J Med Virol 81: 42–48.
Bonadio WA, Smith DS, Goddard S et al. (1990).
Distinguishing cerebrospinal fluid abnormalities in chil-
dren with bacterial meningitis and traumatic lumbar punc-
ture. J Infect Dis 162: 251–254.
Dubos F, Moulin F, Gajdos V et al. (2006a). Serum procalci-
tonin and other biologic markers to distinguish between
bacterial and aseptic meningitis. J Pediatr 149: 72–76.
Dubos F, Lamotte B, Bibi-Triki F et al. (2006b). Clinical deci-
sion rules to distinguish between bacterial and aseptic men-
ingitis. Arch Dis Child 91: 647–650.
Dubos F, De la Rocque F, Levy C et al. (2008). Sensitivity of
the bacterial meningitis score in 889 children with bacterial
meningitis. J Pediatr 152: 378–382.
Kanegaye JT, Soliemanzadeh P, Bradley JS (2001). Lumbar
puncture in pediatric bacterial meningitis: defining the time
interval for recovery of cerebrospinal fluid pathogens after
parenteral antibiotic pretreatment. Pediatrics 108: 1169–1174.
Kimberlin DW, Whitley RJ, Wan W et al. (2011). Oral acyclo-
vir suppression and neurodevelopment after neonatal her-
pes. N Engl J Med: 365: 1284–1292.
Lee BE, Chawla R, Langley JM et al. (2006). Paediatric
Investigators Collaborative Network on Infections in
Canada (PICNIC) study of aseptic meningitis. BMC
Infect Dis 6: 68.
Nigrovic LE, Kuppermann N, Malley R (2002).
Development and validation of a multivariable predictive
model to distinguish bacterial from aseptic meningitis in
children in the post-Haemophilus influenzae era.
Pediatrics 110: 712–719.
Nigrovic LE, Kuppermann N, Macias CG et al. (2007a).
Clinical prediction rule for identifying children with cere-
brospinal fluid pleocytosis at very low risk of bacterial
meningitis. JAMA 297: 52–60.
Nigrovic LE, Kuppermann N, Neuman MI (2007b). Risk fac-
tors for traumatic or unsuccessful lumbar punctures in chil-
dren. Ann Emerg Med 49: 762–771.
Nigrovic LE, Malley R, Macias CG et al. (2008). Effect of
antibiotic pretreatment on cerebrospinal fluid profiles of
children with bacterial meningitis. Pediatrics 122: 726–730.
Nigrovic LE, Malley R, Kuppermann N (2012). Meta-analysis
of bacterial meningitis score validation studies. Arch Dis
Child Jul 4.
Ramers C, Billman G, Hartin M et al. (2000). Impact of a
diagnostic cerebrospinal fluid enterovirus polymerase
chain reaction test on patient management. JAMA 283:
2680–2685.
Rittichier KR, Bryan PA, Bassett KE et al. (2005). Diagnosis
and outcomes of enterovirus infections in young infants.
Pediatr Infect Dis J 24: 546–550.
Torpy JM, Lynm C, Glass RM (2007). JAMA patient page.
Meningitis. JAMA 297: 122.
1156 L.E. NIGROVIC
1
/
4
100%