Insuffisance respiratoire aiguë chez le patient onco

Insuffisance respiratoire aiguë
chez le patient onco-hématologique
Point de vue du réanimateur
Genève, octobre 2009
Pr. Jean-Claude Chevrolet
Soins Intensifs -
Hôpitaux Universitaires de Genève
Suisse

Ce que j’aimerais savoir du réanimateur …
Admission en réanimation
de
mon patient
onco-hématologique
:
.quand ? pourquoi ?
.si mon patient est âgé, cela change-t-il quelque chose ?
.les refus d’admission en réanimation
Que va devenir mon patient
en réanimation ?
.risque de décès ?
.vont-ils “arrêter les machines”
?
.la “réanimation
d’attente “
?

“Just say no”
Carlon GC
Crit Care Med 1989;17:106
“Consider saying yes”
Groeger J
Crit Care Med 2003;31;123
Today ?
…say yes …
but for a limited amount of time
!

0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8 9 10 11 12
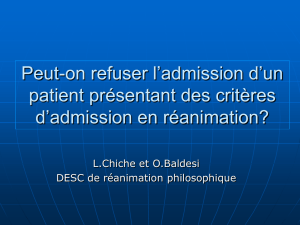
Probability
of
survival after
discontinuation of
mechanical
ventilation -
bone marrow
transplants
months
Crawford S, Am Rev Respir Dis 1988
post ICU percent
survival
rate
hospital discharge
: 4 %
6-months survival
>
tx
: 3 %
ICU survival 26 %

1983
1986
1991
1998
2001
2004
2008
study publication, year
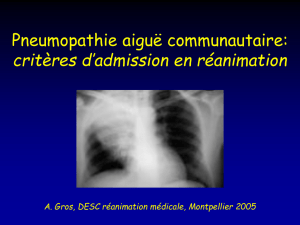
100
80
60
40
20
0
mortality rate, %
Unajusted mortality rate in critically ill cancer
patients by year of study publication
Darmon M et al, Curr Opin Oncol 2009;21:318
> 90 %
> 90 %
< 40 %
< 40 %
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
1
/
74
100%