HEMOTEST

NOTICE D’UTILISATION
HEMOTEST
Ref: 5451
INSTRUCTIONS FOR USE
ALL. DIAG
10, rue Ettoré Bugatti – BP 28006
67038 STRASBOURG Cedex 2 - FRANCE
Tél. : +33 3 88 78 80 88 - Fax : +33 3 88 78 76 78
www.alldiag.com – [email protected]

Liste des Symboles
Attention, voir notice d’utilisation
Tests par coffret
Fabricant
Pour diagnostic in vitro
uniquement Péremption
Usage unique
Conserver entre 4-30°C
No. de lot
REF Code produit
Index of Symbols
Attention, see instructions for use
Tests per kit
Manufacturer
For in vitro
diagnostic use only Use by
Do not reuse
Store between 4-30°C
Lot Number
REF Catalog #
Directive 98/79/CE
Version 10 – Mise à jour le 20/11/2006
ALL. DIAG
10, rue Ettoré Bugatti – BP 28006
67038 STRASBOURG Cedex 2 - FRANCE
Tél. : 03 88 78 80 88 - Fax : 03 88 78 76 78
www.alldiag.com – [email protected]
Fabriquant /
Manufacturer
30
°C
4°C
30°C
4°C

All Diag - 1 - Version 10
HEMOTEST
Trousse de détection de l’hémoglobine humaine dans les selles
Réf. 5451
Pour diagnostic in vitro.
1- INTRODUCTION
La méthode au gaiac développée par Van Deen en 1864 a permis de détecter des traces de sang dans des milieux divers. Dès
1908, Boas utilisa cette méthode pour la mise en évidence de saignement occulte dans les selles. Depuis de nombreux progrès
basés sur la mise en évidence de l’activité péroxydasique de l’hème ont été réalisés. Néanmoins les tests au gaiac impliquent
l’exclusion de certains aliments, médicaments et vitamines, avant et pendant la période de recueil des selles. Certains auteurs
ont également constaté que chez des patients atteints de cancers colorectaux ou d’adénomes, le test au gaiac était négatif par
manque de sensibilité.
Les développements respectifs des méthodes d’agglutination au latex (Adams et al., 1974), d’immunodiffusion radiale
(Songster et al., 1980) et d’hémagglutination reverse (Scito et al., 1984) ont permis la mise au point de tests plus sensibles de
détection de l’hémoglobine humaine dans les selles.
Des études cliniques ont montré que les tests au gaiac donnent des résultats positifs dans 50 à 60% des cas de cancers
colorectaux et seulement 25 à 35% des cas de polypes. De nouvelles méthodes de détection du sang dans les selles sont donc
particulièrement intéressantes pour améliorer le diagnostic et le traitement des maladies à l’origine de saignements occultes.
HEMOTEST a été développé pour mettre en évidence des quantités de sang dans les selles non détectable par les méthodes
au gaiac. Ce test est spécifique de l’hémoglobine humaine et ne nécessite aucun régime ou restriction particulière avant le test.
2- PRINCIPE DU TEST
HEMOTEST est un test immunochromatographique sur membrane utilisant une méthode sandwich de capture.
HEMOTEST contient une combinaison de deux anticorps monoclonaux. Un anticorps monoclonal est conjugué à de l’or
colloïdal, et un second anticorps monoclonal est fixé à la membrane. Si l’échantillon de selles contient de l’hémoglobine, celle-
ci va se lier à l’anticorps marqué à l’or colloïdal et le complexe va migrer le long de la membrane au niveau de la zone test T.
Au niveau de la zone CONTROL ″ C ″, l’anticorps marqué va former une bande de contrôle lorsque le test sera terminé. En 5
minutes ou moins, des quantités d’hémoglobine humaine supérieures ou égales à 20 µg Hb/g de selles sont détectées.
3- COMPOSITION DE LA TROUSSE
1. 20 sachets aluminium contenant les savonnettes ainsi qu’un sachet déssicant. Chaque savonnette contient une membrane
de nitrocellulose coatée au niveau de la zone CONTROL « C » avec un anticorps de chèvre anti souris et au niveau de la
zone TEST « T » avec un anticorps monoclonal de souris anti hémoglobine humaine. Un second anticorps monoclonal
anti hémoglobine humaine est marqué à l’or colloïdal et est situé au dessus du puits échantillon « S ».
2. 20 tubes collecteurs contenant un tampon de dilution.
3. Une notice d’utilisation.
4- MATERIEL NON FOURNI
Chronomètre
5- CONSERVATION ET PEREMPTION
Les sachets aluminium contenant les savonnettes doivent être conservés à température ambiante, entre 4°C et 30°C. Si ils sont
conservés au réfrigérateur attendre que la savonnette revienne à température ambiante avant d’ouvrir le sachet
aluminium. Eviter d’exposer la trousse au chaud ou au froid. NE PAS CONGELER.
Ne pas utiliser au-delà de la date de péremption indiquée sur le coffret.
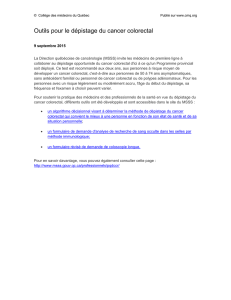
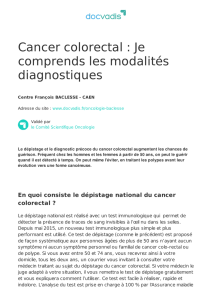
6- PROCEDURE
1. Recueillir un échantillon de selles fraîchement émises dans un récipient propre.
2. Dévisser le capuchon violet du tube collecteur et sortir la tige de recueil.
3. Introduire la tige dans l’échantillon de selles à 6 endroits différents.
4. Si besoin, retirer l’excès de matières fécales déposé sur la tige avec une serviette en papier.
5. Replacer le capuchon violet et visser hermétiquement. L’échantillon ainsi préparé peut être conservé au réfrigérateur (2°C
à 8°C) avant la réalisation du test.

All Diag - 2 - Version 10
6. Agiter énergiquement le collecteur avant d’effectuer le test afin de remettre en suspension.
7. Sortir la savonnette de son sachet aluminium et la poser sur une surface horizontale et plane. Maintenir le tube vertical
avec le capuchon violet vers le haut. Couper l’extrémité de l’embout violet à la main.
8. Déposer 2 à 3 gouttes dans le puits “ S ” par pression sur le corps du tube collecteur.
9. Lire le résultat au bout de 5 minutes. Ne pas lire après 10 minutes.
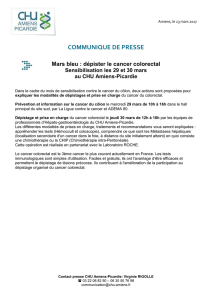
7- RESULTATS
POSITIF : Deux bandes colorées mauves sont visibles au niveau de la zone TEST “ T ” et de la zone contrôle “ C ”.
L’échantillon contient de l’hémoglobine humaine.
NEGATIF: Une seule bande colorée mauve apparaît au niveau de la zone CONTROL “ C ”. L’échantillon ne contient pas
d’hémoglobine humaine en quantités détectables par le test.
Note : Si aucune bande colorée n’apparaît au niveau des zones “ T ” et “ C ”, le test n’a pas fonctionné correctement. Il faut
recommencer à partir d’une nouvelle savonnette. De même, le test n’est pas validé si seule une bande apparaît au niveau de la
zone Test « T ».
8- CONTROLE DE QUALITE
Un contrôle de procédure interne est intégré au test (bande de contrôle « C »). Cela permet de contrôler que le volume de
tampon est suffisant et que la procédure a été suivie correctement.
L’absence de bruit de fond sur la membrane sert de contrôle négatif de procédure interne : Si un bruit de fond important
(coloration mauve importante dans la fenêtre résultat) apparaît et empêche une bonne lecture, le résultat doit être considéré
comme non significatif.
Il est recommandé d’utiliser des contrôles positifs et négatifs pour vérifier les performances du test sur toute nouvelle livraison.
9- CONDITIONS DE CONSERVATION DE L’ECHANTILLON
Les selles à analyser doivent être fraîchement émises. On peut conserver les selles 3 jours à 2-8°C ou 24 heures à température
ambiante. L’hémoglobine humaine contenue dans les selles reste stable dans ces conditions. Une fois l’échantillon de selles
dilué dans le tube collecteur, le mélange peut être conservé 7 jours entre 2°C et 8° C.
Capuchon
Tube
collecteur
3
. Prélever à 6 endroits différents
2
4
5
7
8
1

All Diag - 3 - Version 10
10- PRECAUTIONS
Ne pas utiliser le test au-delà de la date de péremption. Suivre les instructions avec précautions. Pour usage “ in vitro ”
uniquement. Ouvrir le sachet juste avant la réalisation du test. Inscrire le nom et le numéro de dossier du patient directement
sur la savonnette. Pour minimiser le risque d’apparition d’effet crochet, il est recommandé de ne prélever qu’une petite
quantité de selles (de la taille d’une tête d’épingle) en présence de selles sanglantes ou noires. Ne pas manger, boire ou fumer
lors de la manipulation des échantillons et du test. Se munir d’une blouse, de gants et de protection oculaire lors de la
réalisation du test. Eviter les éclaboussures et formation d’aérosol. L’humidité et la température peuvent affecter le résultat du
test. Les échantillons peuvent être contaminés par des agents infectieux. Considérer le matériel directement en contact avec les
échantillons comme des produits contaminés. Traiter ensuite les différents éléments du test et les échantillons selon la
procédure réservée aux déchets potentiellement infectieux.
11- LIMITES DU TEST
1. HEMOTEST est un diagnostic complémentaire pour le médecin. Il ne peut se substituer à l’examen clinique ainsi qu’à la
fibroscopie, l’endoscopie ou à la coloscopie.
2. HEMOTEST ne détecte pas les faibles concentrations d’hémoglobine (<0,2 µg/mL de tampon ou <20µg/g de selles).
Certaines pathologies intestinales (polypes, cancers colorectaux) peuvent entraîner des saignements intermittents ou même
parfois aucun saignement. Le sang peut aussi ne pas être réparti de façon uniforme dans les selles. Ainsi un test peut être
négatif même en présence d’une pathologie.
3. En cas d’hémorroïdes ou d’hématurie ou pendant la période des règles, de faux résultats positifs peuvent être obtenus. Le
recueil de l’échantillon doit être éloigné de plus de trois jours des périodes menstruelles. L’alcool, l’aspirine ou d’autres
médicaments irritants pour l’appareil gastro-intestinal peuvent provoquer des saignements. Leur prise doit être arrêtée au
moins 48 heures avant le recueil des selles.
4. Des résultats positifs peuvent être liés à des pathologies autres que polypes et cancer colorectal (maladie de Crohn,
Rectocolite hémorragique, diarrhées infectieuses, diarrhées parasitaires)
12- PERFORMANCES
1. Sensibilité
La sensibilité analytique d’HEMOTEST est : 0,2µg d’hémoglobine/mL de tampon ou 20 µg d’hémoglobine/g de selles.
2. Spécificité
HEMOTEST est spécifique de l’hémoglobine humaine. Des échantillons positifs et négatifs contenant les substances
suivantes ont été testées sans interférence sur le résultat du test.
SUBSTANCE CONCENTRATION
Hémoglobine de poulet 500 µg/ml
Hémoglobine de porc 500 µg/ml
Hémoglobine de vache 500 µg/ml
Hémoglobine de chèvre 500 µg/ml
Hémoglobine de cheval 500 µg/ml
Hémoglobine de lapin 500 µg/ml
Péroxydase 2000 µg/ml
3. Etude de charge
Une étude de charge a montré l’absence d’effet crochet jusqu’à une concentration de 2.5 mg d’hémoglobine/ml de tampon
de dilution.
4. Reproductibilité
Des échantillons positifs et négatifs ont été testés dans des essais multiples sans qu’aucune discordance n’apparaisse.
5. Corrélation
Dans une étude clinique, 100 échantillons ont été testés avec HEMOTEST et HEMOTOP. 53 échantillons positifs et 47
échantillons négatifs ont été identifiés avec les deux tests.
HEMOTOP
+ -
+ 53 0
HEMOTEST - 0 47
6. Evaluation dans le cadre d’un dépistage généralisé
L’HEMOTEST a été évalué dans le cadre d’une campagne de dépistage de masse sur une population de 26 827 personnes de
plus de 30 ans dans les environs de Pékin (République populaire de Chine). 19 852 personnes se sont soumises entièrement à la
campagne de dépistage soit un taux d’adhésion de 74%. L’âge médian de la population étudiée était de 50 ans. 501 personnes
ont été trouvées positives en HEMOTEST soit un taux de positivité de 5.6% contre 35.36% pour un test au gaïac. Les 501
personnes positives en HEMOTEST ont toutes eu une coloscopie. Des lésions positives ont été trouvées chez 77.8% d’entre
elles.
 6
7
8
9
10
6
7
8
9
10
1
/
10
100%