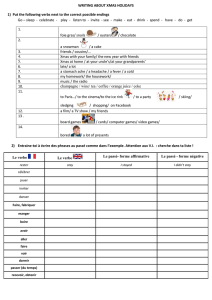
Tabac et maladies inflammatoires de l`intestin

Tabagismeetmaladies
inflammatoiresintestinales
EdouardLouis

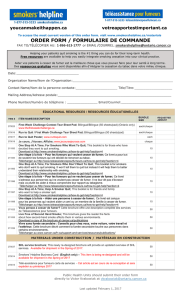
IncreasingincidenceofIBD

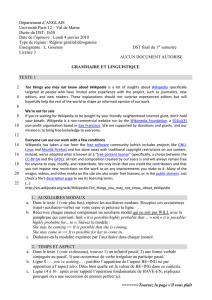
DifférentesfacettesdesMICI

Fracturessur
ostéoporose
Abcèsetfistules
Sténoses
intestinales
Cancercolo‐rectal
Mesalazine
Immunosuppresseurs
Corticoïdes
Antibiotiques
Anti‐TNF

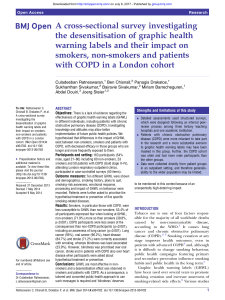
Bactéries‐virus‐flore
Germesspécifiques?
Rupturedetolérance?
Déficitdedéfenseprimairenonspécifique?
 6
7
8
9
10
11
12
13
14
15
16
17
6
7
8
9
10
11
12
13
14
15
16
17
1
/
17
100%