PDF [2iMo]


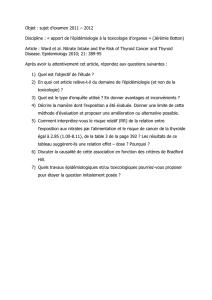
MME. E, 53 ANS
•Africaine, religieuse, sans ATCD particulier
•CMT, stade 2, T2N0M0
(perdue de vue)
2005: CMT 2012: récidive
cervicale + hépatique
2015: céphalées
chirurgie chirurgie RF CEIA
>2500 82 296 1576 1360 693 596 1041 2350
surveillance bio
Calcitonine:
Traitement: ?

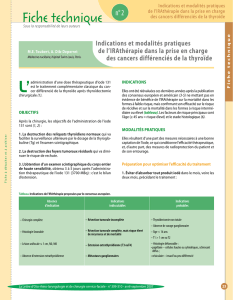
BILAN IMAGERIE
•TDM crane et IV •IRMc: T1 gado T2
méta CMT ? Intérêt d’une TEP-TDM (18)F-FDOPA?
PRECOCE

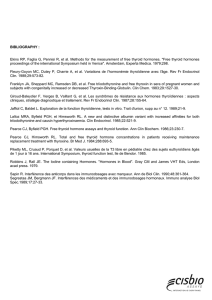
BILAN IMAGERIE
TEP-TDM (18)F-DOPA
Diagnostic = métastase CMT !
PRECOCE TARDIF

METASTASE ORBITAIRE GAUCHE ISOLEE
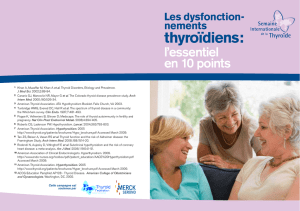
•Biopsie compromise : pas de preuve histologique
•Dgn certitude => (18)F-DOPA +++
•PEC: RTE (IMRT): 40Gy en 20 fractions de 2Gy/sessions -5/7j, 4semaines
•Bonne tolérance clinique
•Surveillance +++ : clinique, imagerie et biologique
•IRM: T1 gado (M0-M1) •IRM: T2 (M0-M1)
=> Stabilité morphologique à 1 mois post-RT
=> Stabilité morphologique à 4 mois post-RT
IRM: T1 gado (M0-M4) IRM: T2 (M0-M4)
•Calcitonine (ng/L) +++
=> Réponse partielle biologique
 6
7
8
6
7
8
1
/
8
100%