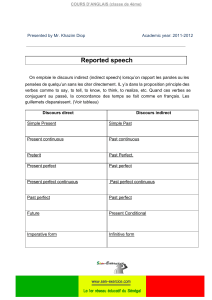
70 ans

GUIDE DE L’EXAMEN MÉDICAL
PÉRIODIQUE
Adolescent - Adulte
NOVEMBRE 2004
Mise à jour : novembre 2006
Préparé par Dre Guylène Thériault
Dre Cléo Mavriplis
UMF Gatineau

Recommandations
Maladies métaboliques et nutritionnelles
Glycémie (dépistage du diabète)
Cholestérol
Tension artérielle
Ostéoporose
TSH
Hemochromatose
Cancers
Sein
Côlon (recherche de sang dans les selles)
Col utérin
Prostate
Testicules
Poumon
Vessie
Ovaires
Pancréas
Oral
Peau
Thyroide
Maladies infectieuses Troubles de la vision ou de l’audition
Chlamydia Vision
Gonorrhée Glaucome
Rubéole Surdité
HIV
Syphilis Santé mentale
Tuberculose Drogues
Bactériurie Dépression
Hepatites Démence
Herpes
Human papilloma virus Santé de la femme
Contraception
Acide folique préconception
Habitudes de vie Chimioprophylaxie pour le
Tabac cancer du sein
Alcool Hormonothérapie
Diète
Obésité
Activité physique
Prévention des accidents
MCAS Aspirine (prévention primaire)
Dépistage
Vitamine E
Maladies vasculaires
Anévrysme de l’aorte abdominale
Sténose carotidienne
MVAS
Annexe 1 Feuilles synthèse des recommandation par sexe et groupe d’âge
Annexe 2 Suggestions de feuilles de prise de données pour l’examen périodique adulte
Annexe 3 Feuilles sommaires
Annexe 4 Critères pour les recommandations des différents groupes
Annexe 5 SCORE, ORAI

Pour chaque thème il y a la recommandation du Groupe d’étude canadien sur les
soins de santé préventifs et/ou celle de son équivalent américain.
Les recommandations de groupes de travail ou d’associations qui semblaient
pertinentes ont aussi été retranscrites. Pour assurer la fiabilité de la
retranscription la langue d’origine a été conservée
L’immunisation n’a pas été abordé. Le PIQ étant selon moi une excellente
référence (souvent mise à jour et fiable)
Les problématiques liées à la grossesse ou aux problèmes dentaires ne sont pas
couvertes
Remerciements à
Dr Gilles Brousseau pour les feuilles sommaires
Dre Guylaine Proulx, Dre Marie-Claude Dupras, Dre Helène Bureau et Dre
Louise Guay pour leurs commentaires
Patricia Rhéaume, Irène Veilleux et Pierre Lebrun pour leur support technique

GLYCÉMIE (dépistage du diabète)
CANADA
1) CTFPHC
2005: There is fair evidence to recommend screening adults with hypertension or
hyperlipidemia for type 2 diabetes mellitus to prevent cardiovascular events and death
(Recommandation B) There is good evidence to recommend lifedtyle interventions for
overweight individuals (BMI>25 or >22 if on asian descent) with impaired glucose tolerance
to reduce the incidence of progression to diabetes (Recommandation B) There is fair
evidence to recommend acarbose treatment for overweight individuals (as above) with
impaired glucose tolerance to prevent cardiovascular events and hypertension
(Recommandation B) There is insufficient evidence to recommend metformin or acarbose
treatment for overweight individuals with impaired glucose tolerance to prevent diabetes
progression (Recommandation I)
1993 : Good evidence to include dipstick screening for protein in the PHE of adults with
IDDM. (Recommandation A)
2) Association canadienne du diabète 2003
Le dépistage du diabète au moyen de l’épreuve de glycémie à jeun doit être fait tous les 3 ans
chez les personnes de 40 ans et plus (Catégorie D, consensus). Des mesures de la glycémie à
jeun ou de la glycémie 2 heures après l’ingestion de 75 g de glucose doivent être effectuées
plus fréquemment et/ou plus tôt chez les personnes qui présentent des facteurs de risque
additionnels de diabète (Catégorie D, consensus ).
ETATS-UNIS
1) USPSTF 2003
The USPSTF concludes that the evidence is insufficient to recommend for or against routinely
screening asymptomatic adults for type 2 diabetes, impaired glucose tolerance, or impaired
fasting glucose. (Recommandation I)
The USPSTF recommends screening for type 2 diabetes in adults with hypertension or
hyperlipidemia. (Recommandation B)
2) American diabetes association 2006
Screening to detect pre-diabetes (IFG or IGT) and diabetes should be considered in
individuals ≥ 45 years of age, particularly in those with a BMI ≥25 kg/m2. Screening should
also be considered for people who are <45 years of age and are overweight if they have
another risk factor for diabetes (• are habitually physically inactive • have a first-degree relative with diabetes • are members
of a high-risk ethnic population (e.g., African American, Latino, Native American, Asian American, Pacific Islander) • have delivered a baby
weighing >9 lb or have been diagnosed with GDM • are hypertensive (140/90 mmHg) • have an HDL cholesterol level <35 mg/dl (0.90
mmol/l) and/or a triglyceride level >250 mg/dl (2.82 mmol/l) • have PCOS • on previous testing, had IGT or IFG • have other clinical
conditions associated with insulin resistance (e.g. PCOS or acanthosis nigricans) • have a history of vascular disease) Repeat testing
should be carried out at 3-year intervals.

CHOLESTÉROL
CANADA
1) CTFPHC 1994
Screening should be considered in all men aged 30 to 59 years; individual clinical judgement should be exercised
in all other cases (Recommandation C) For men 30 to 59 years old with a mean total cholesterol level of more
than 6.85 mmol/L or an LDL-C level of more than 4.50 mmol/L treatment is efficacious in reducing incidence of
CHD. (Recommandation B) For all other asymptomatic individuals the value of treatment has not been
demonstrated. (Recommandation C) Révision en cours?
2) The working group on hypercholesterolemia and other dyslipidemias (Canada)
2003: Routinely screen men over 40 years of age and women who are postmenopausal or over 50 years of age.
In addition screen those with: diabetes mellitus, risk factors such as hypertension, smoking or abdominal obesity;
a strong family history of premature cardiovascular disease; manifestation of hyperlipidemia or evidence of
symptomatic or asymptomatic atherosclerosis 2000 : Although there are no evidence-based recommendations
regarding the optimal frequency for screening, it is reasonable to suggest that asymptomatic patients be screened
every 5 years after the age of 40 for men and 50 for women
3) Association canadienne du diabete 2006
In adults, fasting lipids levels should be measured at the time of diagnosis of diabetes and then every 1 to 3 years
as clinically indicated.
ETATS-UNIS
1) USPSTF 2001
The U.S. Preventive Services Task Force (USPSTF) strongly recommends that clinicians routinely screen men
aged 35 years and older and women aged 45 years and older for lipid disorders and treat abnormal lipids in
people who are at increased risk of coronary heart disease. (Recommendation A)
AAFP has same recommandation (strongly recommands)
The USPSTF recommends that clinicians routinely screen younger adults (men aged 20 to 35 and women aged
20 to 45) for lipid disorders if they have other risk factors for coronary heart disease (Recommandation B)
(Diabetes., A family history of cardiovascular disease before age 50 years in male relatives or age 60 years in
female relatives, A family history suggestive of familial hyper-lipidemia. Multiple coronary heart disease risk
factors (e.g., tobacco use, hypertension).
The optimal interval for screening is uncertain. On the basis of other guidelines and expert opinion, reasonable
options include every 5 years, shorter intervals for people who have lipid levels close to those warranting
therapy, and longer intervals for low-risk people who have had low or repeatedly normal lipid levels
An age to stop screening is not established.
Screening may be appropriate in older people who have never been screened, but repeated screening is less
important in older people because lipid levels are less likely to increase after age 65 years
2) NCEPP III 2001 NCEPP: National cholesterol education program (USA)
In all adults aged 20 years or older, a fasting lipoprotein profile should be obtained once every five years.
(rien de nouveau sur dépistage dans update 2004)The American Heart Association has the same
recommandation
3) AACE 2002 American association of clinical endocrinologists
Screening for dyslipidemia is warranted for all adults up to 75 years of age regardless of CAD risk status and for
adults more than 75 years old who have multiple CAD risk factors (if they have good quality of life and no other
major life-limiting disease).
For adult more than 20 years of age with no CAD risk factors the screening should be done every 5 years. (more
often if CAD risk factors exist)
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
1
/
43
100%