Expression of macrophage migration inhibitory factor in esophageal

Expression of macrophage migration inhibitory factor in esophageal
squamous cell carcinoma and effects of bile acids and NSAIDs
Harry Hua-Xiang Xia
1
, Shu Tian Zhang
2
,
Shiu Kum Lam
1
, Marie Chia-Mi Lin
3
, Hsiang Fu Kung
3
and Benjamin Chun-Yu Wong
1,4
1
Department of Medicine, The University of Hong Kong, Queen Mary
Hospital, Hong Kong,
2
Department of Medicine, Beijing Friendship
Hospital, Capital University of Medical Sciences, Beijing, China and
3
Institute of Molecular Biology, The University of Hong Kong, Hong Kong
4
To whom correspondence should be addressed
Email: [email protected]
The aim of this study was to determine the macrophage
migration inhibitory factor (MIF) protein and mRNA
expression in esophageal squamous cell carcinoma
(ESCC), and the effect of bile acids, aspirin and a selective
cyclooxygenase-2 (COX-2) inhibitor, NS398, on MIF
expression in ESCC cells in vitro. Specimens from tumors
and the adjacent non-cancerous tissues were obtained
from 52 ESCC patients. Western blotting was used for
the detection of MIF protein expression, and reverse
transcription-- polymerase chain reaction (RT-- PCR) for
MIF mRNA expression. Cells of an ESCC cell line, Eca-
109, were treated with chenodeoxycholate (CD, 100 mM),
glycochenodeoxycholate (GCD, 1 mM), aspirin (1 mM) or
NS398 (1 mM). Enzyme-linked immunosorbent assay
(ELISA) and RT-- PCR were used to detect the expression
of the MIF protein and mRNA, respectively, in the super-
natant and cultured cells. Western blotting demonstrated
that levels of MIF protein were increased in tumors versus
non-malignant tissues, with the expression ratio of MIF
over b-actin of 0.93 0.21 and 0.57 0.08, respectively
(P¼0.012). In vitro, both CD and GCD induced a dramatic
increase in MIF protein and mRNA in ESCC cells. On the
other hand, aspirin and NS398 significantly decreased MIF
protein and mRNA expression, and completely blocked bile
acid-induced MIF synthesis in the presence or absence
of prostaglandin E
2
. In conclusion, MIF expression
is increased in ESCC. Whereas bile acids induce MIF
expression in ESCC cells, aspirin and NS398 significantly
inhibit MIF expression, even in the presence of bile acids,
via a COX-independent mechanism.
Introduction
Esophageal cancer is one of the common malignancies, with
an increasing incidence and a high mortality in both developed
and developing countries (1). Esophageal cancer exists in
two main forms with distinct etiological and pathological
characteristics, namely esophageal squamous cell carcinoma
(ESCC) and adenocarcinoma. Whereas adenocarcinoma is
more prevalent in the USA and some other Western countries,
ESCC is the predominant type in the other parts of the world,
especially in Asia, accounting for 490% of esophageal cancer
worldwide (2,3). However, the underlying mechanisms that
determine the biological and molecular behaviors of ESCC
have not been fully elucidated, because most current studies
are focusing on esophageal adenocarcinoma.
Macrophage migration inhibitory factor (MIF) was originally
identified in activated lymphocytes. Macrophages were sub-
sequently found to be an important source (4). MIF inhibits the
migration of macrophages and induces a variety of macro-
phage functions, including adherence and phagocytosis. More-
over, MIF plays a pivotal role in inflammatory and immune
diseases (5). In our previous study, MIF was markedly up-
regulated during acute gastric ulceration in rats, which was
associated with accumulation of macrophages (6). Blockade
with the neutralizing anti-MIF antibody inhibited macrophage
accumulation and MIF up-regulation, indicating an important
pathogenic role of MIF in gastric inflammation and ulceration
(6). In addition, we observed that Helicobacter pylori infection
increased the expression of MIF in gastric epithelial and
inflammatory cells (7). Recent studies have revealed that
MIF may also play a critical role in the development of cancers
as a link between inflammation and tumorigenesis (5,8). MIF is
over-expressed in many tumors, including melanoma, neuro-
blastoma, myelomonocytic leukemia, and cancers of the pros-
tate, breast, lung, colon, liver and stomach (5,8-- 16). However,
the precise role of MIF in carcinogenesis remains unclear.
Studies have shown that reflux of duodenal contents con-
tributes to the development of esophageal cancer, whether
adenocarcinoma or ESCC (17-- 19). Bile acids are likely to be
major contributing factors, with previous studies having
demonstrated that bile acids cause mucosal injury, induce
cyclooxygenase-2 (COX-2) expression, stimulate cell prolif-
eration and promote tumorigenesis (20). On the other hand, a
protective role of aspirin and non-steroidal anti-inflammatory
drugs (NSAIDs) in the development of both esophageal adeno-
carcinoma and ESCC has been reported (21).
We hypothesize that MIF expression is increased in ESCC,
and that bile acids, aspirin and NSAIDs are involved in the
regulation of MIF. Therefore, this study was carried out to
determine the expression of MIF protein and mRNA in
patients with ESCC, and the effects of conjugated and uncon-
jugated bile acids, aspirin and a selective COX-2 inhibitor
on MIF expression in esophageal squamous carcinoma cells
in vitro.
Materials and methods
Patients
Fifty-two ESCC patients [39 males and 13 females, with a mean age of 58.9
years (range, 34-- 81)] who underwent surgical treatment without preoperative
therapy in the Department of Surgery, Beijing Friendship Hospital, The Capital
University of Medical Sciences, between January 1999 and December 2002,
Abbreviations: CD, chenodeoxycholate; COX-2, cyclooxygenase-2; ESCC,
esophageal squamous cell carcinoma; GCD, glycochenodeoxycholate; MIF,
migration inhibitory factor; NSAIDs, non-steroidal anti-inflammatory drugs;
RT-- PCR, reverse transcription-- polymerase chain reaction.
Carcinogenesis vol.26 no.1 #Oxford University Press 2005; all rights reserved. 11
Carcinogenesis vol.26 no.1 pp.11-- 15, 2005
doi:10.1093/carcin/bgh279

were included in the study. Surgical treatment consisted of resection of the
esophagus with lymph node dissection. Specimens from tumors and from
adjacent normal-appearing tissues (at least 5 cm away from the tumor) were
obtained from each patient, and immediately frozen in liquid nitrogen.
Cell culture and treatment with chenodeoxycholate, glycochenodeoxycholate,
aspirin and NS398 in the presence or absence of prostaglandin E
2
An ESCC cell line, Eca-109 (22; kindly provided by Prof. G.R.Yang, Henan
Institute of Medical Sciences, Henan Medical University, Zhengzhou, China)
was grown in DMEM containing 10% fetal calf serum (FCS) with 100 U/ml
penicillin and 100 mg/ml streptomycin in a 5% CO
2
atmosphere at 37C. Bile
acids, chenodeoxycholate (CD, 100 mM, Sigma Chemical, St Louis, MO) or
glycochenodeoxycholate (GCD, 1 mM, Sigma), aspirin (1 mM, Sigma) or a
selective COX-2 inhibitor, NS398 (1 mM, Biomol, Plymouth Meeting, PA),
were added to medium containing 1% FCS for 24 h, in the presence or absence
of prostaglandin E
2
(2.8 mM). The concentrations for the bile acids were
selected according to a previous study (20), and also from pilot experiments
where a wide range of concentrations were evaluated. Concentrations chosen
were those that induced MIF protein expression by ~2-fold. There was no
obvious toxicity from these substances, as assessed by measuring the cell
number, trypan blue exclusion and the release of lactate dehydrogenase (data
not shown).
Western blot
Frozen tissue was sliced and thawed in ice-cold RIPA buffer (PBS with 1%
Nonidet P-40, 0.5% sodium deoxycholate and 0.1% SDS) containing protease
inhibitor mixture, with 3 ml RIPA buffer per gram of tissue. The tissue was
homogenized, kept on ice for 30 min and centrifuged twice at 10 000 r.p.m.
for 10 min at 4C. The supernatant was collected and protein content in
the supernatant was measured using a bicinchoninic acid reagent (Pierce,
Rockford, IL). Protein (25-- 30 mg) was electrophoresed using a 10% denatur-
ing SDS gel, and transferred onto an Immobilon-P membrane (Millipore,
Bedford, MA). Blots were incubated with an anti-MIF monoclonal antibody
(R&D Systems, Minneapolis, MN), followed by a horseradish peroxidase-
conjugated anti-IgG antibody (Santa Cruz, CA). The immunoblot bands were
developed and visualized by enhanced chemiluminescence (Amersham,
Piscataway, NJ) and autoradiography. The intensity of the bands was
quantified by densitometry, with b-actin monoclonal antibody (Santa Cruz)
as a control.
Semi-quantitative reverse transcription-- polymerase chain reaction
Total RNA was isolated from frozen tissues as well as cultured cells using the
RNeasy Mini Kit (QIAGEN, Valencia, CA). Semi-quantitative reverse tran-
scription-- polymerase chain reaction (RT-- PCR) was performed using oligo
(dT) as the random primer for reverse transcription and specific MIF primers
and b-actin primers for PCR. Briefly, total RNA was reverse transcribed using
Moloney murine leukemia virus reverse transcriptase (QIAGEN) at a concen-
tration of 2 U/mg for 2 h at 42C. PCR was carried out using QuantiTECTTM
SYBR PCR Kit (QIAGEN). The following primers were used to amplify a
185-bp fragment of MIF: sense primer, 50-GTT CCT CTC CGA GCT CAC
CCA GCA GC-30; antisense primer, 50-GCA GCT TGC TGT AGG AGC GGT
TCT G-30. Primers for the amplification of human b-actin mRNA were as
follows: sense primer, 50-ATG GAA TTC CCG TGG AAC AAG AAT GAG
ATC AG-30; antisense primer, 50-CGT CAT ACT CCT GCT TGC TGA TCC
ACA TCA GC-30. The amplification profile for MIF was 28 cycles of 45-s
denaturation at 95C and 1-min annealing, 1-min extension at 63C, followed
by extension for 5 min at 63C. For b-actin, the amplification profile was 35
cycles of 1-min denaturation at 94C and 1-min annealing at 56C and 1-min
extension at 72C, followed by extension for 5 min at 72C. Afterwards, the
PCR products were resolved on a 1.7% agarose gel, stained with ethidium
bromide, and analyzed by densitometry. Data are expressed using an MIF
expression ratio, which was defined as the MIF band area intensity divided
by the b-actin band area intensity.
Enzyme-linked immunosorbent assay
MIF in the supernatants was measured by enzyme-linked immunosorbent
assay (ELISA) according to the manufacturer’s instruction (R&D Systems).
Briefly, 100 ml of capture anti-human MIF antibody (2 mg/ml) in phosphate-
buffered saline (PBS, pH 7.4) was transferred to each well of an ELISA plate,
and blocked with 1% BSA. 100 ml of each sample, or recombinant human MIF
(R&D Systems) were added, in triplicate, into corresponding wells for 2 h at
room temperature. Biotinylated anti-human MIF antibody (0.2 mg/ml, R&D
Systems) was added and incubated for 2 h at room temperature. After plates
were washed three times, 100 ml streptavidin-HRP (R&D System) at a dilution
of 1 in 200 was added to each well. Following washing for a further four times,
100 ml of a 1:1 mixture of reagents A (H
2
O
2
) and B (tetramethylbenzidine) was
added. Finally, the reaction was stopped by adding 50 mlH
2
SO
4
. Absorbance
was read using a microtiter plate reader (NovaPathTM, Bio-Rad, Hercules, CA)
at 450 nm.
Statistical methods
Data obtained from the study were expressed as the mean SD. Statistical
analysis was performed using SPSS software (version 10.0, SPSS, Chicago,
IL). Independent-sample t-test and the Mann-- Whitney U-test, where appro-
priate, were used to determine the differences between numeric variables.
The Pvalues calculated were two-tailed. The alpha level of significance was
set at P50.05.
Results
Expression of MIF protein in tumor and the corresponding
non-malignant tissues
Western blotting of ESCC tumor and the corresponding non-
malignant specimens demonstrated the expected band for MIF
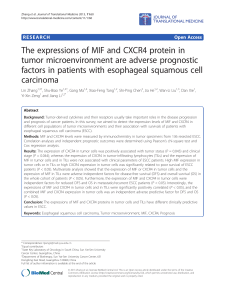
protein with a molecular weight of 12.5 kDa. In 50 of 52 cases
(96.15%), the expression levels of MIF protein were higher
in tumors than in the corresponding non-malignant tissues
(Figure 1). Overall, the mean expression ratio of MIF over
b-actin was 0.93 0.21 for tumor samples and 0.57 0.08 for
the corresponding non-malignant tissues (n¼52, P¼0.012).
Expression of MIF mRNA in tumor and the corresponding
non-malignant tissues
Further, RT-- PCR analysis showed that MIF mRNA was
expressed both in the tumor and in the corresponding non-
malignant tissues, but the expression levels were higher in the
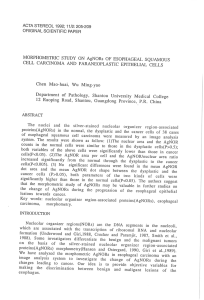
former than in the latter for 48 of 52 cases (92.31%) (Figure 2).
The mean ratio of the MIF mRNA band area intensity divided
Fig. 2. Representative RT-- PCR analysis showing higher levels of MIF
mRNA expression in ESCC tumor (T) than in the corresponding
non-malignant, normal-appearing tissue (N).
Fig. 1. A representative western blot showing higher levels of MIF protein
expression in ESCC tumor (T) than in the corresponding non-malignant,
normal-appearing tissue (N).
H.H.-X.Xia et al.
12

by the b-actin mRNA band area intensity was 0.82 0.12 for
tumors and 0.34 0.05 for the corresponding non-malignant
tissue (n¼52, P¼0.011).
Effect of CD, GCD, aspirin and NS398 on MIF protein and
mRNA expression in esophageal squamous carcinoma cells in
the presence or absence of prostaglandin E
2
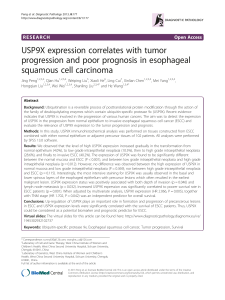
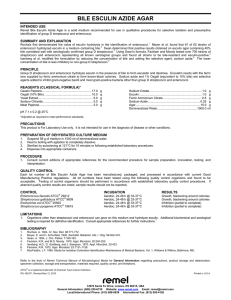
Both CD and GCD induced a dramatic increase in MIF protein
and mRNA expression in the esophageal squamous carcinoma
cells in vitro (Figure 3). On the other hand, aspirin and NS398
significantly decreased the MIF protein and mRNA expres-
sion. Moreover, aspirin and NS398 completely blocked bile
acid-mediated induction of MIF synthesis at both protein and
mRNA levels (Figures 3 and 4). However, the inhibitory effect
of aspirin and NS398 was not reversed by addition of prosta-
glandin E
2
, and prostaglandin E
2
did not have any impact on
MIF expression (Figure 3).
Discussion
In the present study, the expression of MIF protein and mRNA
was significantly increased in ESCC, compared with the
corresponding non-malignant tissues, suggesting that MIF is
involved in the pathogenesis of ESCC. Further investigation is
required to elucidate the underlying mechanisms, although
promotion of cell proliferation, tumor angiogenesis and meta-
stasis has been implicated (9,13,23-- 25).
Duodenogastroesophageal reflux, exposing esophageal tissue
to acid, pepsin, bile and pancreatic juices play a significant
role in the development of Barrett’s metaplasia and esophageal
carcinoma, and refluxed duodenal contents per se cause
esophageal carcinoma in rats (17-- 19). Bile acids within the
duodenal contents are likely to be major contributing factors in
tumorigenesis through mucosal injury and stimulation of cell
proliferation (20,26,27). In explants of Barrett’s esophagus
ex vivo and in esophageal adenocarcinoma cells, bile acids
up-regulate COX-2 expression and prostaglandin E (PGE)
release, and increase cell proliferation (20,28-- 30). In cultured
esophageal squamous carcinoma cells, bile acids also signifi-
cantly increase COX-2 expression and PGE release, with the
unconjugated bile acid, CD, being more potent than the con-
jugated bile acid, GCD (20). In the present study, both bile
acids significantly stimulated MIF expression at both protein
and mRNA levels in cultured esophageal squamous carcinoma
cells, suggesting that bile acids promote esophageal squamous
carcinoma cells, at least in part, through an MIF-mediated
pathway (i.e. involving MIF-mediated cell proliferation and
angiogenesis).
Aspirin/NSAIDs are protective against both esophageal
adenocarcinoma and ESCC, probably through inhibition of
COX activity, with subsequent stimulation of apoptosis and
suppression of cell growth (21,31-- 38). In addition, aspirin/
NSAIDs may also reduce the incidence of esophageal cancers
by decreasing esophageal inflammation, which is a risk factor
for both esophageal adenocarcinoma and ESCC (39,40). In the
present study, we observed that both aspirin and the COX-2
inhibitor, NS398, decreased MIF expression in the esophageal
squamous carcinoma cells. Moreover, the effect of aspirin/
NSAIDs on MIF expression was not influenced by addition
of bile acids, with stimulatory effect of bile acids on MIF
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
Control CD GCD Aspirin NS398 CD/Aspirin CD/NS398 GCD/Aspirin GCD/NS398
Average levels of MIF expression (pg/ml)
Without PGE2
With PGE2
*
*
*
*
**
*
*
*
*
*
*
*
*
*
*
Fig. 3. Effect of CD, GCD, aspirin and NS398, with and without prostaglandin E
2
, on MIF protein expression in ESCCs in vitro. The bar represents the SD.
P50.001, compared with the control.
Fig. 4. Effect of CD, GCD, aspirin and NS398 on MIF mRNA expression in
esophageal cancer cells in vitro as demonstrated by RT-- PCR analysis.
MIF in esophageal squamous cell carcinoma
13

expression being completely blocked by aspirin/NSAIDs.
These findings further support the notion that aspirin and
NSAIDs play a protective role in the pathogenesis of esopha-
geal cancer including ESCC, and suggest that regulation of
MIF expression by aspirin and the COX-2 inhibitor, contribute
to this protective role. A few studies have looked at the asso-
ciation between MIF and COX-2 (41,42). One such study
reported that recombinant human MIF up-regulated COX-2
mRNA, and anti-MIF monoclonal antibody significantly
reduced COX activity and mRNA expression (42). It has
been shown that MIF inhibits p53 activity, and importantly,
that this regulation coincides with the induction of arachidonic
acid metabolism and COX-2 expression (43,44). The latter
supported our initial hypothesis that inhibition of MIF-induced
COX-2 activity by aspirin/NSAIDs might contribute to the
protective role of these drugs in the development of ESCC.
However, our further experiment indicates that aspirin/
NSAIDs modulate MIF expression by a COX-independent
mechanism, because addition of prostaglandin E2 in the
culture medium did not reverse the inhibitory effect of
aspirin/NSAIDs.
Further studies are required to determine the exact mechan-
isms by which aspirin/NSAIDs inhibit bile acid-induced MIF
expression. It has been demonstrated that bile acids activate
protein kinase K and the transcription factors AP-1 and NF-
kB, induce IL-8 expression and up-regulate some oncogenes
such as c-myc in esophageal adenocarcinoma cells (45-- 48).
Therefore, it would be helpful to determine whether bile acids
exert similar effects in esophageal squamous carcinoma cells
and whether aspirin/NSAIDs inhibit bile acid-induced MIF
expression by antagonizing one or more of these pathways.
In addition, it is generally accepted that cigarette smoking and
alcohol intake are closely associated with the development of
ESCC, an association that may account for 90% of ESCC cases
in the developed world (49). There is evidence that one of the
molecular targets for cigarette smoking is the p53 gene, and
damage to this gene is known to depend on the number of
cigarettes smoked per day (50). It is possible that cigarette
smoking exerts its effect on p53 through an MIF-mediated
pathway, but this hypothesis needs to be tested further.
In conclusion, MIF expression is increased in ESCC.
Whereas bile acids induce MIF expression in esophageal squa-
mous carcinoma cells, aspirin and NS398, a COX-2 inhibitor,
significantly inhibit MIF expression even in the presence of
bile acids, in a COX-independent mechanism.
Acknowledgements
This project was supported by a competitive earmarked research grant from the
Research Grants Council of Hong Kong Special Administrative Region, China
(HKU7318/01 M to H.H.-X.X.). S.T.Z. was a visiting professor sponsored by
the Croucher Foundation (Chinese Visitorship Scheme), The University of
Hong Kong. The authors thank Dr Hua He and Dr Yun Wei Sun, Department
of Medicine, The University of Hong Kong, Hong Kong, and Dr Xing Xiang
He, Department of Medicine, The Second Affiliated Hospital of Guangzhou
Medical College, Guangzhou, China, for technical assistance.
References
1. Pisani,P., Parkin,D.M., Bray,F. and Ferlay,J. (1999) Estimates of the
world-wide mortality from 25 cancers in 1990. Int. J. Cancer,83,18-- 29.
2. Souza,R.F. (2002) Molecular and biologic basis of upper gastrointestinal
malignancy-- esophageal carcinoma. Surg. Oncol. Clin. North. Am.,11,
257-- 272.
3. Stoner,G.D. and Gupta,A. (2001) Etiology and chemoprevention of
esophageal squamous cell carcinoma. Carcinogenesis,22, 1737-- 1746.
4. Calandra,T., Bernhagen,J., Mitchell,R.A. and Bucala,R. (1994) The
macrophage is an important and previously unrecognized source of
macrophage migration inhibitory factor. J. Exp. Med.,179, 1895-- 1902.
5. Lue,H., Kleemann,R., Calandra,T., Roger,T. and Bernhagen,J. (2002)
Macrophage migration inhibitory factor (MIF): mechanisms of action and
role in disease. Microb. Infect.,4, 449-- 460.
6. Huang,X.R., Hui,C.W.C., Chen,Y.X. et al. (2001) Macrophage migration
inhibitory factor is an important mediator in the pathogenesis of gastric
inflammation in rats. Gastroenterology,121, 619-- 630.
7. Xia,H.H.X., Lam,S.K., Huang,X.R., Wong,W.M., Leung,S.Y., Yuen,S.T.,
Lan,H.Y. and Wong,B.C.Y. (2004) Helicobacter pylori infection is
associated with increased expression of macrophage migration inhibitory
factor by epithelial cells, T cells and macrophages in gastric mucosa.
J. Infect. Dis.,190, 293-- 302.
8. Bucala,R. (2000) A most interesting factor. Nature,408, 167-- 168.
9. Shimizu,T., Abe,R., Nakamura,H., Ohkawara,A., Suzuki,M. and
Nishihira,J. (1999) High expression of macrophage migration inhibitory
factor in human melanoma cells and its role in tumor cell growth and
angiogenesis. Biochem. Biophys. Res. Commun.,264, 751-- 758.
10. Bin,Q., Johnson,B.D., Schauer,D.W., Casper,J.T. and Orentas,R.J. (2002)
Production of macrophage migration inhibitory factor by human and
murine neuroblastoma. Tumour Biol.,23, 123-- 129.
11. Meyer-Siegler,K. (2000) Increased stability of macrophage migration
inhibitory factor (MIF) in DU-145 prostate cancer cells. J. Interferon
Cytokine Res.,20, 769-- 778.
12. Bando,H., Matsumoto,G., Bando,M., Muta,M., Ogawa,T., Funata,N.,
Nishihira,J., Koike,M. and Toi,M. (2002) Expression of macrophage
migration inhibitory factor in human breast cancer: association with nodal
spread. Jpn. J. Cancer Res.,93, 389-- 396.
13. Takahashi,N., Nishihira,J., Sato,Y., Kondo,M., Ogawa,H., Ohshima,T.,
Une,Y. and Todo,S. (1998) Involvement of macrophage migration
inhibitory factor (MIF) in the mechanism of tumor cell growth. Mol.
Med.,4, 707-- 714.
14. Kamimura,A., Kamachi,M., Nishihira,J., Ogura,S., Isobe,H., Dosaka-
Akita,H., Ogata,A., Shindoh,M., Ohbuchi,T. and Kawakami,Y. (2000)
Intracellular distribution of macrophage migration inhibitory factor
predicts the prognosis of patients with adenocarcinoma of the lung.
Cancer,89, 334-- 341.
15. Akbar,S.M., Abe,M., Murakami,H., Tanimoto,K., Kumagi,T.,
Yamashita,Y., Michitaka,K., Horiike,N. and Onji,M. (2001) Macrophage
migration inhibitory factor in hepatocellular carcinoma and liver cirrhosis;
relevance to pathogenesis. Cancer Lett.,171, 125-- 132.
16. He,X.X., Xia,H.H.X., Yang,Y. et al. (2003) Increased serum levels and
epithelial expression of macrophage migration inhibitory factor in gastric
cancer. Gastroenterology,124, A556 (abstract).
17. Goldstein,S.R., Yang,G.Y., Curtis,S.K., Reuhl,K.R., Liu,B.C.,
Mirvish,S.S., Newmark,H.L. and Yang,C.S. (1997) Development
of esophageal metaplasia and adenocarcinoma in a rat surgical
model without the use of a carcinogen. Carcinogenesis,18, 2265-- 2270.
18. Miwa.K., Sahara,H., Segawa,M., Kinami,S., Sato,T., Miyazaki,I. and
Hattori,T. (1996) Reflux of duodenal or gastro-duodenal contents induces
esophageal carcinoma in rats. Int. J. Cancer,67, 269-- 274.
19. Pera,M., Brito,M.J., Poulsom,R., Riera,E., Grande,L., Hanby,A. and
Wright,N.A. (2000) Duodenal-content reflux esophagitis induces the
development of glandular metaplasia and adenosquamous carcinoma in
rats. Carcinogenesis,21, 1587-- 1591.
20. Zhang,F., Altorki,N.K., Wu,Y.C., Soslow,R.A., Subbaramaiah,K. and
Dannenberg,A,J. (2001) Duodenal reflux induces cyclooxygenase-2 in the
esophageal mucosa of rats: evidence for involvement of bile acids.
Gastroenterology,121, 1391-- 1399.
21. Corley,D.A., Kerlikowske,K., Verma,R. and Buffler,P. (2003) Protective
association of aspirin/NSAIDs and esophageal cancer: a systematic review
and meta-analysis. Gastroenterology,124,47-- 56.
22. Tang,H. and Yang,X.P. (2002) Effect of boanmycin on apoptosis and cell
cycle of human esophageal cancer (Eca-109) cells. Aizheng,21, 855-- 859
(Chinese).
23. Chesney,J., Metz,C., Bacher,M., Peng,T., Meinhardt,A. and Bucala,R.
(1999) An essential role for macrophage migration inhibitory factor (MIF)
in angiogenesis and the growth of a murine lymphoma. Mol. Med.,95,
181-- 191.
24. Yang,Y., Degranpre,P., Kharfi,A. and Akoum,A. (2000) Identification of
macrophage migration inhibitory factor as a potent endothelial cell
growth-promoting agent released by ectopic human endometrial cells.
J. Clin. Endocrinol. Metab.,85, 4721-- 4727.
H.H.-X.Xia et al.
14

25. Ogawa,H., Nishihira,J., Sato,Y., Kondo,M., Takahashi,N., Oshima,T. and
Todo,S. (2000) An antibody for macrophage migration inhibitory factor
suppresses tumour growth and inhibits tumour-associated angiogenesis.
Cytokine,12, 309-- 314.
26. Craven,P.A., Pfanstiel,J. and DeRubertis,F.R. (1987) Role of activation of
protein kinase C in the stimulation of colonic epithelial proliferation and
reactive oxygen formation by bile acids. J. Clin. Invest.,79, 532-- 541.
27. Reddy,B.S., Watanabe,K., Weisburger,J.H. and Wynder,E.L. (1977)
Promoting effect of bile acids in colon carcinogenesis in germ-free and
conventional F344 rats. Cancer Res.,37, 3238-- 3242.
28. Shirvani,V.N., Ouatu-Lascar,R., Kaur,B.S., Omary,M.B. and
Triadafilopoulos,G. (2000) Cyclooxygenase 2 expression in Barrett’s
esophagus and adenocarcinoma: ex vivo induction by bile salts and acid
exposure. Gastroenterology,118, 487-- 496.
29. Kaur,B.S. and Triadafilopoulos,G. (2002) Acid- and bile-induced PGE(2)
release and hyperproliferation in Barrett’s esophagus are COX-2 and
PKC-epsilon dependent. Am. J. Physiol. Gastrointest. Liver Physiol.,
283, G327-- G334.
30. Zhang,F., Subbaramaiah,K., Altorki,N. and Dannenberg,A.J. (1998)
Dihydroxy bile acids activate the transcription of cyclooxygenase-2.
J. Biol. Chem.,273, 2424-- 2428.
31. Ratnasinghe,D., Tangrea,J., Roth,M.J., Dawsey,S., Hu,N., Anver,M.,
Wang,Q.H. and Taylor,P.R. (1999) Expression of cyclooxygenase-2 in
human squamous cell carcinoma of the esophagus; an immunohistochem-
ical survey. Anticancer Res.,19, 171-- 174.
32. Morris,C.D., Armstrong,G.R., Bigley,G., Green,H. and Attwood,S.E.
(2001) Cyclooxygenase-2 expression in the Barrett’s metaplasia-
dysplasia-adenocarcinoma sequence. Am. J. Gastroenterol.,96, 990-- 996.
33. Fosslien,E. (2000) Molecular pathology of cyclooxygenase-2 in neoplasia.
Ann. Clin. Lab. Sci.,30,3-- 21.
34. Zhu,G.H., Wong,B.C., Eggo,M.C., Ching,C.K., Yuen,S.T., Chan,E.Y.,
Lai,K.C. and Lam,S.K. (1999) Non-steroidal anti-inflammatory drug-
induced apoptosis in gastric cancer cells is blocked by protein kinase
C activation through inhibition of c-myc. Br. J. Cancer,79, 393-- 400.
35. Zhou,X.M., Wong,B.C., Fan,X.M., Zhang,H.B., Lin,M.C., Kung,H.F.,
Fan,D.M. and Lam,S.K. (2001) Non-steroidal anti-inflammatory drugs
induce apoptosis in gastric cancer cells through up-regulation of bax and
bak. Carcinogenesis,22, 1393-- 1397.
36. Jiang,X.H., Lam,S.K., Lin,M.C., Jiang,S.H., Kung,H.F., Slosberg,E.D.,
Soh,J.W., Weinstein,I.B. and Wong,B.C. (2002) Novel target for induction
of apoptosis by cyclo-oxygenase-2 inhibitor SC-236 through a protein
kinase C-beta(1)-dependent pathway. Oncogene,21, 6113-- 6122.
37. Li,M., Lotan,R., Levin,B., Tahara,E., Lippman,S.M. and Xu,X.C. (2000)
Aspirin induction of apoptosis in esophageal cancer: a potential for
chemoprevention. Cancer Epidemiol. Biomarkers Prev.,9, 545-- 549.
38. Souza,R.F., Shewmake,K., Beer,D.G., Cryer,B. and Spechler,S.J. (2000)
Selective inhibition of cyclooxygenase-2 suppresses growth and induces
apoptosis in human esophageal adenocarcinoma cells. Cancer Res.,60,
5767-- 5772.
39. Morgan,G.P. and Williams,J.G. (1994) Inflammatory mediators in the
oesophagus. Gut,35, 297-- 298.
40. Chang-Claude,J.C., Wahrendorf,J., Liang,Q.S., Rei,Y.G., Munoz,N.,
Crespi,M., Raedsch,R., Thurnham,D.I. and Correa,P. (1990) An epide-
miological study of precursor lesions of esophageal cancer among young
persons in a high-risk population in Huixian, China. Cancer Res.,50,
2268-- 2274.
41. Meyer-Siegler,K. (2001) COX-2 specific inhibitor, NS-398, increases
macrophage migration inhibitory factor expression and induces neuro-
endocrine differentiation in C4-2b prostate cancer cells. Mol. Med.,7,
850-- 860.
42. Sampey,A.V., Hall,P.H., Mitchell,R.A., Metz,C.N. and Morand,E.F.
(2001) Regulation of synoviocyte phospholipase A2 and cyclooxygenase
2 by macrophage migration inhibitory factor. Arth. Rheumat.,44,
1273-- 1280.
43. Hudson,J.D., Shoaibi,M.A., Maestro,R., Carnero,A., Hannon,G.J. and
Beach,D.H. (1999) A proinflammatory cytokine inhibits p53 tumor
suppressor activity. J. Exp. Med.,190, 1375-- 1382.
44. Mitchell,R.A., Liao,H., Chesney,J., Fingerle-Rowson,G., Baugh,J.,
David,J. and Bucala,R. (2002) Macrophage migration inhibitory factor
(MIF) sustains macrophage proinflammatory function by inhibiting p53:
regulatory role in the innate immune response. Proc. Natl Acad. Sci. USA,
99, 345-- 350.
45. Fitzer,C.J., O’Brian,C.A., Guillem,J.G. and Weinstein,I.B. (1987) The
regulation of protein kinase C by chenodeoxycholate, deoxycholate and
several structurally related bile acids. Carcinogenesis,8, 217-- 220.
46. Glinghammar,B., Inoue,H. and Rafter,J.J. (2002) Deoxycholic acid causes
DNA damage in colonic cells with subsequent induction of caspases,
COX-2 promoter activity and the transcription factors NF-kB and AP-1.
Carcinogenesis,23, 839-- 845.
47. Jenkins,G.J., Harries,K., Doak,S.H., Wilmes,A., Griffiths,A.P., Baxter,J.N.
and Parry,J.M. (2004) The bile acid deoxycholic acid (DCA) at neutral pH
activates NF-kappaB and induces IL-8 expression in oesophageal cells
in vitro.Carcinogenesis,25, 317-- 323.
48. Tselepis,C., Morris,C.D., Wakelin,D., Hardy,R., Perry,I., Luong,Q.T.,
Harper,E., Harrison,R., Attwood,S.E. and Jankowski,J.A. (2003)
Upregulation of the oncogene c-myc in Barrett’s adenocarcinoma:
induction of c-myc by acidified bile acid in vitro.Gut,52, 174-- 180.
49. Enzinger,P.C. and Mayer,R.J. (2003) Esophageal cancer. N. Engl. J. Med.,
349, 2241-- 2252.
50. Mizobuchi,S., Furihata,M., Sonobe,H., Ohtsuki,Y., Ishikawa,T.,
Murakami,H., Kurabayashi,A., Ogoshi,S. and Sasaguri,S. (2000)
Association between p53 immunostaining and cigarette smoking in
squamous cell carcinoma of the esophagus. Jpn. J. Clin. Oncol.,30,
423-- 428.
Received December 9, 2003; revised February 3, 2004;
accepted August 31, 2004
MIF in esophageal squamous cell carcinoma
15
1
/
5
100%