a v a i l a b l e a... j o u r n a l h o m...

Epidemiology, Staging, Grading, and Risk Stratification of
Bladder Cancer
Marc Colombel
a,
*, Mark Soloway
b
, Hideyuki Akaza
c
, Andreas Bo
¨hle
d
, Joan Palou
e
,
Roger Buckley
f
, Donald Lamm
g
, Maurizio Brausi
h
, J. Alfred Witjes
i
, Raj Persad
j
a
Department of Urology, Claude Bernard University, Ho
ˆpital Edouard Herriot, Lyon, France
b
Department of Urology, University of Miami School of Medicine, Miami, Florida, USA
c
Department of Urology, University of Tsukuba, Tsukuba, Japan
d
Department of Urology, HELIOS Agnes Karll Hospital, Bad Schwartau, Germany
e
Department of Urology, Fundacio
´Puigvert, Universitat Auto`noma de Barcelona, Barcelona, Spain
f
Department of Urology, North York General Hospital, Toronto, Ontario, Canada
g
Department of Surgery, University of Arizona; BCG Oncology, Phoenix, Arizona, USA
h
Department of Urology, AUSL Modena Estense and B Ramazzini Hospitals, Modena, Italy
i
Department of Urology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands
j
Department of Urology/Surgery, Bristol Royal Infirmary and Bristol Urological Institute, Bristol, United Kingdom
european urology supplements 7 (2008) 618–626
available at www.sciencedirect.com
journal homepage: www.europeanurology.com
Article info
Keywords:
Bladder cancer risk factors
Epidemiology
Grading
Non–muscle invasive
bladder cancer
Risk stratification
Staging
Please visit
www.eu-acme.org/
europeanurology to read and
answer questions on-line.
The EU-ACME credits will
then be attributed
automatically.
Abstract
Context: Understanding the epidemiology and risk factors for non–muscle invasive blad-
der cancer (NMIBC) can assist in the prevention and early detection of the disease.
Furthermore, staging, grading, and risk stratification are critical for determining the most
appropriate management strategies for NMIBC based on risk of recurrence and progres-
sion.
Objective: To provide community urologists with an overview of the epidemiology of
NMIBC as well as current approaches to staging, grading, and risk stratification.
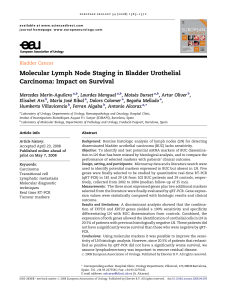
Evidence acquisition: A committee of internationally renowned leaders in bladder cancer
management, known as the International Bladder Cancer Group (IBCG), identified current
key influencing guidelines and published English-language literature related to the
epidemiology, staging, and grading of NMIBC available as of March 2008. The IBCG met
on four occasions to review the main findings of the identified literature and the current
clinical practice guidelines of the European Association of Urology (EAU), the First
International Consultation on Bladder Tumors (FICBT), the National Comprehensive
Cancer Network (NCCN), and the American Urological Association (AUA).
Evidence synthesis: Based on this review, the IBCG provided a summary on the epidemiol-
ogy of NMIBC and recommendations for the staging, grading, and risk stratification of the
disease.
Conclusions: Urologists should record the smoking habits of patients and monitor for
possible occupational exposure to urothelial carcinogens. The tumour-node-metastases
(TNM) classification for tumour staging and both the World Health Organization (WHO)
1973 and 2004 grading systems should be applied for appropriate staging and grading of
NMIBC. Urologists should also consider the use of the European Organisation for Research
and Treatment of Cancer (EORTC) risk tables for risk stratification of NMIBC based on risk
of disease recurrence and progression.
#2008 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Service D’Urologie – CHU Edouard Herriot, 5 place d’Arsonval,
cedex 03, 69437 Lyon, France. Tel. +33 472 11 62 89; Fax: +33 472 11 05 82.
E-mail address: [email protected] (M. Colombel).
1569-9056/$ – see front matter #2008 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eursup.2008.08.002

1. Introduction
A thorough understanding of the epidemiology of
bladder cancer can assist in the prevention and early
detection of the disease. In addition, staging, grading,
and risk stratification are essential for determining
the most appropriate management strategies for
non–muscle invasive bladder cancer (NMIBC) based
on risk of recurrence and progression. Therefore, a
committee of internationally renowned leaders in
bladder cancer management, known as the Interna-
tional Bladder Cancer Group (IBCG), identified current
key influencing guidelines and published English-
language literature related to the epidemiology,
staging, and grading of NMIBC available as of March
2008. The IBCG met on four occasions to review the
main findings of the identified literature and the
current clinical practice guidelines of the European
Association of Urology (EAU), the First International
Consultation on Bladder Tumors (FICBT), the
National Comprehensive Cancer Network (NCCN),
and the American Urological Association (AUA). This
article provides a summary of the epidemiology of
NMIBC and the IBCG’s recommendations for staging,
grading, and risk stratification of the disease based on
currently available guidelines and evidence.
2. Incidence
Bladder cancer ranks ninth in worldwide cancer
incidence. It is the 7th most common cancer in men
and the 17th most common cancer in women [1].
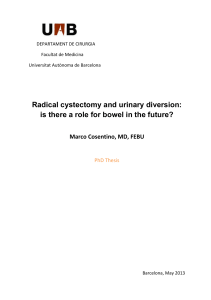
Globally, the incidence of bladder cancer varies
significantly, with Egypt, Western Europe, and North
America having the highest incidence rates, and
Asian countries the lowest rates (see Fig. 1)[2].
Although the disease may occur in young persons,
>90% of new cases occur in persons 55 yr of age [3].
3. Risk factors
Thetwomostwell-establishedriskfactorsfor bladder
tumours are cigarette smoking and occupational
exposure to urothelial carcinogens [4,5]. Cigarette
smoking is the most important riskfactor, accounting
for 50% of cases in men and 35% in women [5]. In fact,
cigarette smokers have a 2- to 4-fold increased risk of
bladder cancer compared to non-smokers [6],and
the risk increases with increasing intensity and/or
duration of smoking [7]. Upon cessation of cigarette
smoking, the risk of bladder cancer falls >30% after
1–4 yr and >60% after 25 yr [7,8] but never returns to
the level of risk of non-smokers.
Occupational exposure to urothelial carcinogens
is the second most important risk factor, accounting
for 5–20% of all bladder cancers [9,10]. The relative
risk of occupational exposure to carcinogens is likely
underestimated and varies from country to country.
Current or historical exposure to aromatic amines
(eg, benzidine, 2-naphthylamine, 4-aminobiphenyl,
o-toluidine, and 4-chloro-o-toluidine) used in the
chemical, rubber, and dye industries [11–13] and
polycyclic aromatic hydrocarbons (PAHs) used in the
aluminum, coal, and roofing industries [14] have all
been associated with the development of bladder
cancer. An increased risk of bladder cancer has also
been reported in painters, varnishers, and hair-
dressers [15].
Other environmental exposures that have been
associated with bladder cancer include chronic
urinary tract infections [16], cyclophosphamide
use [17], and exposure to radiotherapy [18]. Recently,
the Cancer of the Prostate Strategic Urologic
Research Endeavor (CaPSURE) group found an
increased incidence of bladder cancer in men with
prostate cancer treated with radiotherapy [19].
Inadequate consumption of fruits, vegetables,
and certain vitamins may also play a role in the
development of bladder cancer. A meta-analysis by
Steinmaus et al [20] found that increased risks of
bladder cancer were associated with diets low in
fruit intake (relative risk [RR], 1.40; 95% confidence
interval [CI], 1.08–1.83), and slightly increased risks
were associated with diets low in vegetable intake
(RR, 1.16; 95% CI, 1.01–1.34). Evidence also suggests
that garlic [21] and vitamin A [22] have chemo-
protective effects in bladder cancer. Furthermore, a
small randomised study of 65 patients with transi-
tional cell carcinoma (TCC) of the bladder found that
megadoses of vitamins A, B6, C, and E plus zinc
decreased bladder tumour recurrence in patients
receiving bacillus Calmette-Gue
´rin (BCG) immu-
notherapy [23]. Large-scale prospective, randomised
trials are required to clarify the role of vitamins in
bladder cancer prevention.
Although it has been suggested that coffee
consumption and artificial sweeteners may be asso-
ciated with an increased risk of bladder cancer,
results from epidemiologic studies investigating
these agents have been inconclusive. A major
problem in evaluating the independent effect of
coffee consumption on the development of bladder
cancer is its relationship to cigarette smoking [1].To
avoid the residual confounding effect of cigarette
smoking, a pooled analysis of studies examining non-
smokers in Europe was performed. Although the
study was limited by bias in control selection, the
investigators observed a significant increased risk of
european urology supplements 7 (2008) 618–626 619

bladder cancer only in subjects consuming 10 cups
of coffee per day (odds ratio [OR], 1.8; 95% CI, 1.0–3.3)
[24]. Furthermore, most epidemiologic studies have
failed to show any evidence of bladder carcinogeni-
city with saccharin and other sweeteners [1]. In 1999,
the International Agency for Research on Cancer
(IARC) concluded that saccharin and its salts were not
classifiable as carcinogenic in humans, despite
evidence suggesting that sodium saccharin causes
urothelial bladder tumours in experimental animals
[25].
Familial bladder cancer is rare compared to the
familial occurrence of cancer in other tumour sites.
However, there does appear to be an increased risk
Fig. 1 – Worldwide age-standardised incidence rates (per 100 000) for bladder cancer in (a) males and (b) females [2].*
* Reprinted from Ferlay et al [2].
european urology supplements 7 (2008) 618–626620

of bladder cancer in individuals with a family history
of cancer, particularly in those with first-degree
relatives who developed bladder cancer at age 60 yr
or earlier [26]. A population-based, family case-
control study by Aben et al [27] found an almost
2-fold increased risk among first-degree relatives of
patients with urothelial cell carcinoma, which could
not be explained by smoking. A segregation analysis
of >1100 families could not find strong evidence of
inheritance of bladder cancer through a single major
gene. However, the investigators could not exclude
the possibility of an inherited subtype of bladder
cancer. A major gene may segregate in some
families, but this effect may have been masked in
a background of high sporadic incidence [28].
4. Major pathologic subtypes
TCC is the most common primary pathologic
subtype of bladder cancer and is observed in >90%
of tumours [29]. Squamous cell carcinoma and
adenocarcinoma are less common and occur in
approximately 5% and 1% of bladder cancers,
respectively [30,31]. Secondary carcinomas can
appear in the colon, uterus, ovaries, and prostate,
as well as lymphomas.
In certain regions of the world where schistoso-
miasis (also known as bilharziasis) infection is
endemic, squamous cell carcinoma can account for
up to 75% of bladder cancers [32,33]. Schistosomiasis
is a parasitic disease caused by various species of
flatworm. It typically affects agricultural commu-
nities, particularly those dependent upon irrigation
to support their agriculture. Areas with a high
prevalence of schistosomiasis include Africa, the
Caribbean, South America, East Asia, and the
Middle East.
Recently, variants of TCC (nested and micropa-
pillary) have been noted that may have prognostic
and therapeutic significance [34,35]. Results from a
recent study suggest that intravesical therapy may
be ineffective in patients with the micropapillary
variant, and that radical cystectomy may be the
preferred treatment option for patients with this
form of TCC [36]. However, Gaya et al [37] recently
noted good results with intravesical BCG in patients
with a micropapillary pattern and without conco-
mitant carcinoma in situ (CIS).
5. Staging and grading
Stage and grade are significant prognostic factors for
recurrence, progression, and survival and, therefore,
are critical for the appropriate treatment and
management of NMIBC.
5.1. Staging
The most widely used and universally accepted
staging system is the tumour-node-metastases
(TNM) system shown in Table 1 [38]. Under this
system, NMIBC includes (1) papillary tumours
confined to the epithelial mucosa (stage Ta); (2)
tumours invading the subepithelial tissue (ie,
lamina propria; T1); and (3) Tis (CIS).
5.2. Grading
Traditionally, bladder carcinomas have been graded
according to the World Health Organization (WHO)
1973 grading of urothelial papilloma: well differ-
entiated (G1), moderately differentiated (G2), or
poorly differentiated (G3). In 2004, the WHO and
Table 1 – 2002 TNM classification of urinary bladder
cancer [38]
T: Primary tumour
TX Primary tumour cannot be assessed
T0 No evidence of primary tumour
Ta Non-invasive papillary carcinoma
Tis Carcinoma in situ: ‘‘flat tumour’’
T1 Tumour invades subepithelial
connective tissue
T2 Tumour invades muscle
T2a: Tumour invades superficial muscle
(inner half)
T2b: Tumour invades deep muscle
(outer half)
T3 Tumour invades perivesical tissue:
T3a: Microscopically
T3b: Macroscopically
T4 Tumour invades any of the following:
prostate, uterus, vagina, pelvic wall,
abdominal wall
T4a: Tumour invades prostate, uterus,
or vagina
T4b: Tumour invades pelvic wall or
abdominal wall
N: Lymph nodes
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single lymph node 2cm
in greatest dimension
N2 Metastasis in a single lymph node >2cm
but not >5 cm in greatest dimension, or
multiple lymph nodes, none >5cmin
greatest dimension
N3 Metastasis in a lymph node >5cmin
greatest dimension
M: Distant metastasis
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
european urology supplements 7 (2008) 618–626 621

the International Society of Urological Pathology
(ISUP) published a new grading system that employs
specific cytologic and architectural criteria [39,40].
The new WHO/ISUP classification differentiates
between papillary urothelial neoplasms of low
malignant potential (PUNLMP) and low-grade and
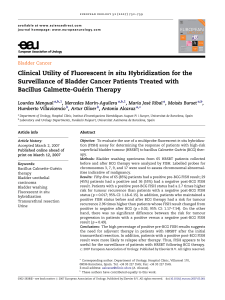
high-grade urothelial carcinomas. Comparisons of
the 1973 and 2004 classification systems are shown
in Table 2 and Fig. 2 [41].
Use of the 2004 WHO/ISUP classification should
result in more uniform diagnoses of tumours that
are better stratified according to risk potential.
However, according to the EAU guidelines for non–
muscle invasive disease, both the 1973 and 2004
WHO classifications should be used for tumour
grading until the 2004 grading system is validated in
more clinical trials [42,43].
Evidence suggests that the WHO/ISUP 2004 classi-
fication does not increase the inter-observer repro-
ducibility of non–muscle invasive tumours compared
to the 1973 WHO classification. Reproducibility is
particularly low for the 2004 PUNLMP classification
(50%). However, differentiation between low-grade
and high-grade urothelial carcinoma using the 2004
classification does have a high inter-observer repro-
ducibility (84–90%) [44–46].
Urologists should interact with their pathologists
to determine which grading system they are using.
Regardless of the grading method utilised, it is
important that the urologist review the pathology
slides with the pathologist.
6. Risk stratification and progression
Approximately 75–80% of bladder tumours present
as non–muscle invasive disease and the remainder
present as muscle-invasive disease [47]. In NMIBC,
approximately 70% present as Ta lesions, 20% as T1
lesions and 10% present as CIS or Tis lesions [6].
NMIBC represents a heterogeneous group of
tumours with completely different oncologic
outcomes. Low-grade tumours, for example, have a
modest recurrence rate but are at low risk for
progression. High-grade tumours, on the other hand,
are associated with significant recurrence, progres-
sion, and mortality rates.
This heterogeneity in bladder tumours compli-
cates the ability to compare the efficacy of different
treatment modalities and thereby establish unified
treatment recommendations. Therefore, risk strati-
fication is imperative for classifying patients with
similar risks of recurrence and progression, and it
helps to determine the appropriate management
strategies for each risk category.
To date, the European Organisation for Research
and Treatment of Cancer (EORTC) risk tables are
considered the most reliable tools for estimating
progression and/or recurrence of NMIBC. The EORTC
scoring system combines data on previous tumour
recurrence rate, number of tumours, tumour dia-
Table 2 – World Health Organization (WHO) grading of
urinary tumours in 1973 and 2004 [39,40]
WHO 1973
Urothelial papilloma
Grade 1: well differentiated
Grade 2: moderately differentiated
Grade 3: poorly differentiated
WHO 2004
Urothelial papilloma
PUNLMP
Low-grade papillary urothelial carcinoma
High-grade papillary urothelial carcinoma
PUNLMP = papillary urothelial neoplasms of low malignant
potential.
Fig. 2 – Comparison of the 1973 and 2004 World Health Organization (WHO) grading systems.
Some 1973 WHO grade 1 carcinomas are reassigned to the papillary urothelial neoplasm of low malignant potential
(PUNLMP) category and others to the 2004 WHO low-grade carcinoma category. Similarly, 1973 WHO grade 2 carcinomas
are reassigned, some to the low-grade carcinoma category and others to the high-grade carcinoma category. All 1973 WHO
grade 3 tumours are assigned to the 2004 WHO high-grade carcinoma category.
TCC = transitional cell carcinoma.
Reprinted with permission from Elsevier Inc [41].
european urology supplements 7 (2008) 618–626622
 6
7
8
9
6
7
8
9
1
/
9
100%