S2-3 Parenteral&OralImmunization_DrSchumacher

1
Criteria for the use of parenteral and oral immunization of dogs
Introduction
Parenteral
and oral
vaccination
Conclusions and
recommendations
Carolin L. Schumacher, International Federation of Animal Health

2
Introduction
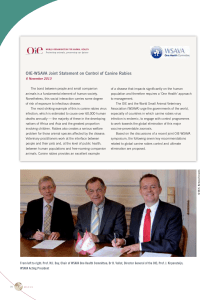
Central-point campaigns in northern Tanzania - Dog registration, vaccination, fitting of temporary collars and issue of vaccination
certificates for each vaccinated dog
Advertising of campaigns in
northern Tanzania

3
Vaccination is a highly effective method for preventing rabies
•Many national rabies vaccination programs started after WW2 have allowed to
eliminate canine rabies from entire countries and even continents:
Japan, Taiwan, Singapore (in the 1950s)
Europe and the USA (by 1970)
•Wildlife rabies prevalence has been reduced in North America and large parts of
Western Europe have been declared free of terrestrial wildlife rabies following years of
large scale application oral vaccination:
Finland, The Netherlands (1991), Italy (1997 ), Switzerland (1998), France
(2000), Belgium, Luxembourg (2001), the Czech Republic (2004), Germany
(2008) and Austria (2008)
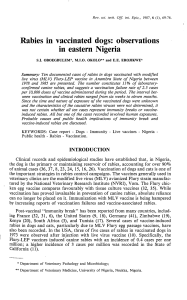
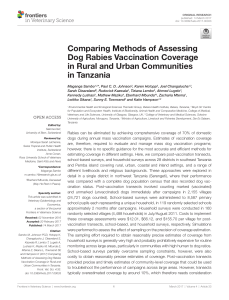
•Canine mass vaccination programs in countries
still affected by canine rabies have significantly
reduced the number of animal and human rabies cases
in many countries of Latin America, Asia and Africa
•Other programs are less advanced and many struggle with logistics and
implementation and thus, tragically, canine rabies continues to claim the majority of
the 55 000 human lives each year
7.17.5 9.1 9.3 9.7 10.6
10.911.112.613.313.7
14.915.916.2 16 16.6
0 0 2
10
3
7
20
15
22
45
29
60
20 19
0
0
2
4
6
8
10
12
14
16
18
1990
19911992199319941995
19961997199819992000
20012002200320042005
0
10
20
30
40
50
60
70
Rabies in Humans, and canine
rabies vaccination,
Mexico, 1990 - 2005
Dogs Vaccinated
Millions
Rabies
Cases

4
The components of a successful canine rabies control program are known
•Knowledge about rabies and its epidemiology
•Clear governance and coordinated mandates among national agencies and stakeholders
•Adequate legislation, sustainable infrastructure and funds available
•Appropriate surveillance and knowledge about rabies epidemiology
•Knowledge of the dog population
•Appropriately trained personnel and accurately used equipment
•Community awareness and involvement
•Sufficient quantities of appropriate supplies and materials
•Dog vaccination campaigns and humane dog population management (if necessary)
•Objective program evaluation
•Adequate measures in place to assure disease freedom
Blueprint for Rabies Prevention and Control
(www.rabiesblueprint.com).
Comprehensive guidelines developed over the last 50 years by experts panels of the
WHO, CDC, GARC, and the OIE are available for most aspects of dog rabies control
rechercheSearch

Vaccines –a critical element of a canine vaccination program
A key factor cited regularly for the success of dog rabies control program is the use of
potent canine rabies vaccines
However, depending on
•which type of vaccine is used
•how the vaccines are produced and stored
•how they are handled and administered
•which type of animal is targeted
•the frequency of vaccination campaigns
•the number and distribution of animals that are reached
•The immune response generated in individuals and the population
•and how campaign success is measured
dog rabies vaccination may produce highly variable results.
rechercheSearch
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
1
/
21
100%