HARNESSING THE IMMUNE SYSTEM TO TREAT AND PREVENT DISEASE JANUARY 2014

HARNESSING THE IMMUNE
SYSTEM TO TREAT AND
PREVENT DISEASE
JANUARY 2014
CSE/OMX:BAVA, OTC:BVNRY

BAVARIAN NORDIC
CANCER IMMUNOTHERAPIES AND VACCINES FOR INFECTIOUS DISEASES
2
FACTS
BAVARIAN NORDIC IN BRIEF
•Vertically integrated multinational biotech company
•Revenue-generating
•Leader in vector-based active immunotherapy – two technology platforms
•First product approved in 2013
•Two Phase 3 programs: Prostate cancer and smallpox
•Ebola vaccine license and supply agreement with Janssen
•Commercial scale cGMP manufacturing facility
•Long-term contracts with the US government
•Founded 1994, IPO 1998
•Headquartered in Denmark
•Research centers in Mountain View, CA
and Munich, Germany
•Listed on NASDAQ OMX Copenhagen: BAVA
REVENUES AND RESULTS, 5 YEARS
-500
0
500
1.000
2009 2010 2011 2012 2013 2014E

3
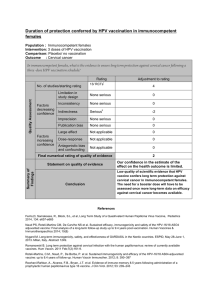
PIPELINE
1) Government funded programs
2) Sold to government stockpiles
3) Approved in the European Union under the trade name IMVANEX® and in
Canada under the trade name IMVAMUNE®
4) Phase 3 registration studies are ongoing in the United States
5) Licensed to Janssen
Preclinical
Phase 1 Phase 1/2 Phase 2 Phase 3 Market
IMVANEX®/ IMVAMUNE® 1-4) Smallpox
PROSTVAC® Prostate Cancer
IMVAMUNE® freeze-dried 1) Smallpox
CV-301 Colon 1) Colorectal Cancer
CV-301 Bladder 1) Bladder Cancer
CV-301 Breast 1) Breast Cancer
MVA-BN® PRO Prostate Cancer
MVA-BN® HER2 Breast Cancer
MVA-BN® Brachyury 1) Metastatic Tumors
MVA-BN® Filo 5) Filoviruses (Ebola/Marburg)
MVA-BN® RSV Respiratory Syncytial Virus
MVA-BN® FMDV 1) Foot-and-mouth Disease
MVA-BN® Anthrax 1) Anthrax

4
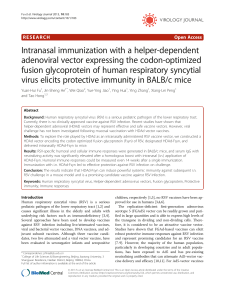
THE MVA-BN® VACCINE PLATFORM
Vaccine Platform
Approvals in EU and Canada
Balanced Immune Response
Strong IP Protection
MVA-BN Antigen(s)
+
Research & Development
Construct Optimization
Immune Enhancement
Preclinical Analysis
Manufacturing
Research Drug Product
Clinical Batch Production
Commercial Manufacturing
MVA-BN
(IMVAMUNE)
Recombinant
MVA-BN

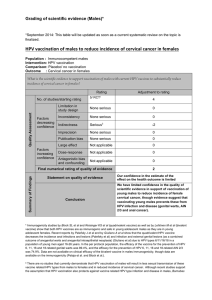
POXVIRUS TECHNOLOGY PLATFORM
5
Vaccinia + Fowlpox (VF)
(Prime) (Boost)
TRICOM
TRIad of CO-stimulatory Molecules
PSA MUC-1 CEA
•Prostate cancer
PROSTVAC CV-301
LFA-3 ICAM-1 B7.1
•Colorectal, Breast, Lung,
Ovarian, Gastric, Bladder, Liver
and Renal cancer
GM-CSF can be used as adjuvant in both PROSTVAC® and CV-301
Immune Targets
(Antigens)
Vectors
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
1
/
28
100%