H Noncommunicable Diseases: An overview of Africa’s new silent killers

AFRICAN HEALTH MONITOR
January-June 2008
2
Noncommunicable Diseases:
An overview of Africa’s new
silent killers
Introduction
Heart disease, stroke, cancer,
diabetes and other chronic
diseases are often thought to be public
health problems of significance only
in high-income countries. In reality,
only 20% of chronic disease deaths
occur in high-income countries, while
80% occur in low- and middle-income
countries where most of the world’s
populations live.1
Moreover, as described in detail in the
WHO publication “Preventing chronic
diseases: a vital investment,” the impact
of chronic diseases in many low- and
middle-income countries is steadily
growing. In these countries, around
28 million people died in 2005 from
a chronic disease, and cardiovascular
disease alone killed five times as many
people as HIV/AIDS. In these settings,
middle-aged adults are especially
vulnerable to chronic disease. Thus,
people tend to develop disease at
younger ages, suffer longer and die
sooner than those in high-income
countries. This undermines countries’
economic development as many of
those affected are at the peak of their
productive and economic activity.
Noncommunicable diseases are the major cause of death and
disability worldwide. The WHO African Region has not been
spared this global epidemic. Noncommunicable diseases are
debilitating and often present fatal complications such as blindness,
renal failure and gangrene leading to lower limb amputations and
hemiplegic conditions. In the Region, chronic diseases are projected
to account for more than a quarter of all deaths by 2015.2
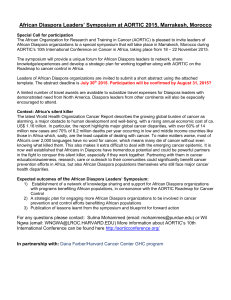
Chronic disease mortality
Noncommunicable diseases, the silent killers, have insidious onset,
provide debilitating complications and result in painful deaths. The
estimated number of chronic disease-related deaths in the WHO
African Region in 2005 was 2 446 0001, 2 (see Figure 1 for other
estimates).
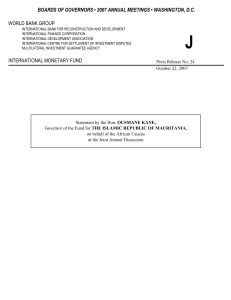
WHO projects that 28 million people in the Region will die from a
chronic disease over the next 10 years. The rate of increase of deaths
from chronic diseases will outstrip that from infectious diseases,
maternal and perinatal conditions, and nutritional deficiencies
more than four-fold in the next 10 years. Most significantly, deaths
from diabetes will increase by 42%.1
* Dr Matshidiso Moeti

AFRICAN HEALTH MONITOR
January-June 2008
3
Figure 1: Projected deaths by cause, all ages,
WHO African Region, 2005
Morbidity related to chronic diseases
The burden of illness from chronic diseases in the Region is already
significant and is set to increase considerably in the next decades,
adding to the overwhelming and unmet demand for health services
due to communicable diseases. The health care burden will be of
a different scale, given the chronic course and the need for long-
term and often life-long treatment.
Cancer
Cancer is an emerging and increasingly
serious public health problem in the
WHO African Region. Existing data
(Globocan 2002) suggest that there
were 582 000 new cancer cases in
sub-Saharan Africa in 2002.3 The
most common cancers recorded were
cervical cancer (12%), breast cancer
(10%), liver cabcer (8%), Karposi’s
sarcoma (5%), non-Hodgkin’s
lymphoma (5%) and prostate cancer
(5%). In 2007, overall, the most
frequently observed cancers were
Kaposi’s sarcoma and liver cancer. The
commonest cancers in males were
Kaposi’s sarcoma and cancers of the
liver and prostate; in females, Kaposi’s
sarcoma and cancers of the cervix and
breast were observed most frequently.
Globally, with appropriate interventions
and services, one third of cancers can be
prevented, one third are curable while
the remaining one third are incurable.
The situation in Africa is quite different:
by the time of diagnosis, 80% to 90%
of patients have incurable cancers, with
only 10% to 15% being curable when
given appropriate treatment.3 This
clearly shows that populations in the
Region are not benefiting from primary
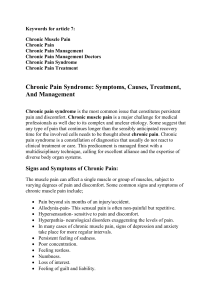
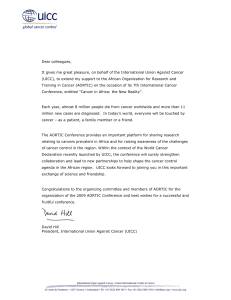
prevention and cure. In 2002, cancer
deaths were estimated at 412 100 in
sub-Saharan Africa. If interventions to
intensify and scale up prevention and
treatment are not put in place, it is
projected that in the year 2020 there
will be 804 000 new cancer cases and
626 400 cancer-related deaths (see
Figure 2).
Figure 2: New cases of cancer annually

AFRICAN HEALTH MONITOR
January-June 2008
4
The main risk factors for cancer
are infections such as HIV/AIDS,
human papillomavirus, hepatitis,
or schistosomiasis; tobacco use;
environmental pollution; unhealthy diet;
excessive alcohol intake; old age; and
lack of physical exercise. Prevention
offers the most cost-effective long-
term strategy for cancer control.
Preventive measures are doubly
beneficial as they can also contribute to
preventing noncommunicable diseases
that share the same risk factors, such as
cardiovascular diseases and diabetes.
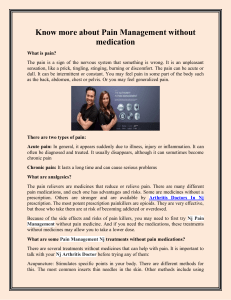
Diabetes
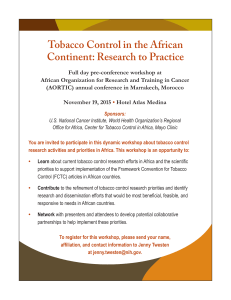
Diabetes mellitus is no longer rare
in Africa (Figure 3). Meta-analytic
estimates and recent investigations
based on the WHO STEPwise
approach to monitoring risk factors for
noncommunicable diseases indicate a
mean estimated prevalence of 2.8%
in 2000, ranging from 1% in some
countries such as Ethiopia, Madagascar,
Mali and Niger among others, to as high
as 20% in Mauritius and Seychelles.
The overall regional prevalence is
projected to reach 4.8% in 2030.3
The total number of persons affected
globally is projected to rise from 171
million in 2000 to 366 million in 2030
if prevention measures are not scaled
up. In Africa, the number of people
with diabetes in 2006 was 10.4 million,
expected to increase to 18.7 million in
2025.
The majority of cases of diabetes in
Africa go undetected; the undiagnosed
cases are estimated to be as high as
60% to 80% in Cameroon, Ghana and
Tanzania.5 Undiagnosed diabetes evolves silently into complications
such as renal failure, retinopathies, foot disease and disease of
the heart. Between 1.4% and 6.7% of diabetic foot cases result
in amputation. Annual mortality linked to diabetes worldwide is
estimated at more than one million. In some countries in Africa, the
mortality rate is very high, more than 40 per 10 000 inhabitants.
Figure 3: Diabetes prevalence rate in the WHO African
Region
Cardiovascular diseases
Hypertension is a main physiological risk factor for other
cardiovascular diseases (CVDs). It is estimated that more than 20
million people are affected in the African Region, mainly in urban
areas. Prevalence ranges from 25% to 35% in adults aged 25 to
64 years.5 Some studies reveal a clear relationship between level of
blood pressure, salt and fat consumption, and body weight. Studies
in Ghana, Mauritius, South Africa and Zimbabwe show an increase
in stroke mortality that could be related to increasing levels of
hypertension, obesity, tobacco use and diabetes. Prevention and
control of hypertension could avoid at least 250 000 deaths per
year.6
Stroke is a major cause of death and the biggest single cause of
disability worldwide. Annually, 15 million people suffer a stroke.
Of these, 5 million die and another 5 million are left permanently
disabled, placing a heavy burden on individuals, families and
communities. The African Region has not been spared.

AFRICAN HEALTH MONITOR
January-June 2008
5
Rheumatic heart disease is the most important form of acquired
CVD in children and adolescents in sub-Saharan Africa. Several
studies show a prevalence of rheumatic heart disease of 15–20 per
1000 population.6 Of the 18 million people currently affected by
rheumatic fever or rheumatic heart disease, two thirds are children
between 5 and 15 years of age.6 There are around 300 000 deaths
each year, with 2 million people requiring repeated hospitalization
and 1 million likely to require surgery in the next 5 to 20 years.5
The impact of this disease on patients, families, health systems and
society is severe.
The increasing burden of CVDs and other chronic diseases in Africa
has not been accompanied by corresponding adjustments in health
service structures, human resources and service delivery modes.
Current health care systems were developed to provide acute,
episodic care. They are inadequately designed and resourced to
care for people with chronic conditions such as CVD, who require
repeated visits, information and counselling on lifestyle changes to
minimize complications and support with adherence to treatment
and self-care.
Conclusion
The WHO African Region now faces a double burden of disease.
While combating communicable diseases, countries are now
confronted with noncommunicable diseases (NCDs) which are
projected to increase significantly. They are related to risk factors
linked mainly to lifestyles which must be dealt with simultaneously.
The NCD burden is likely to be even more untenable in the future
if interventions are not immediately intensified and scaled up in
countries. Investment in this effort now will yield considerable
benefits if the projected morbidity and mortality due to chronic
noncommunicable diseases are averted.
The WHO Regional Office for Africa strongly advocates for and will
support Member States to scale up actions, particularly primary
prevention interventions and other cost-effective interventions, in
NCD management. These actions need to start immediately.
References
1 WHO, Preventing Chronic Diseases:
a vital investment, Geneva, World
Health Organization, 2005.
2 WHO, Noncommunicable diseases:
a strategy for the African Region
(AFR/RC50/10), Brazzaville, World
Health Organization, Regional Office
for Africa, 1990.
3 WHO, Cancer prevention and
control in the WHO African Region
(AFR/RC57/RT/1), Brazzaville,
World Health Organization, Regional
Office for Africa, 2007.
4 WHO, Diabetes prevention and
control: A strategy for the WHO
African Region (AFR/RC57/7),
Brazzaville, World Health
Organization, Regional Office for
Africa, 2007.
5 WHO, Cardiovascular diseases
in the African Region: current
situation and perspectives (AFR/
RC55/12), Brazzaville, World Health
Organization, Regional Office for
Africa, 2005.
6 WHO, Cardiovascular diseases
in the African Region: current
situation and perspectives (AFR/
RC55/12), Brazzaville, World Health
Organization, Regional Office for
Africa, 2005.
* Dr Moeti is the Director, Division
of Prevention and Control of
Noncommunicable Diseases at the
WHO Regional Office for Africa.
1
/
4
100%