Lire l`article

SERVICE PUBLIC HOSPITALIER, PARCOURS, TERRITOIRES,
QUESTIONS POSÉES
1
Séminaire de Palerme!
30 & 31 Mai 2014

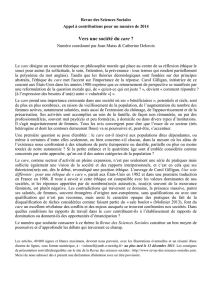
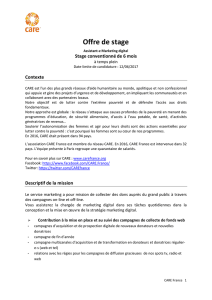
les apports attendus du STS
Loi HPST
ETAT
ARS
ARS
ARS
ARS
ARS
ARS
Loi 2014
ARS
ARS
territoire
ARS
territoire
territoire
territoire
Territorialisation ascendante Régionalisation descendante
2

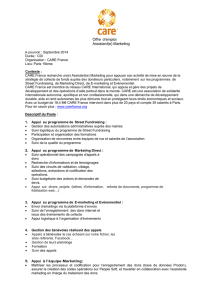
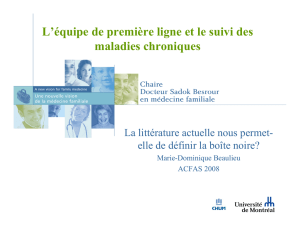
SPH : un bloc de services
Soins
Information en santé
Enseignement, formation / Recherche
Veille sanitaire
Prévention, Santé publique
Disparition des 14 MSP
Intégrationdansmissionsd’intérêtgénéralrevisitées
3

SPH : des principes de service public
accessibilité
continuité
adaptabilité
neutralité
égalité
4

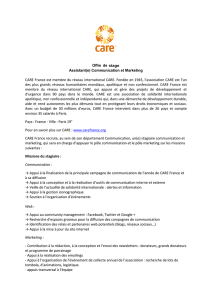
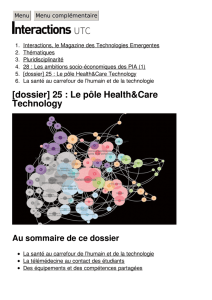
SPH : des règles à observer
Permanence de
soins
Accessibilité
financière
Transparence des
comptes
Participation des
usagers
Maîtrise des
délaisd’attente
5
 6
7
8
9
10
11
12
13
14
6
7
8
9
10
11
12
13
14
1
/
14
100%