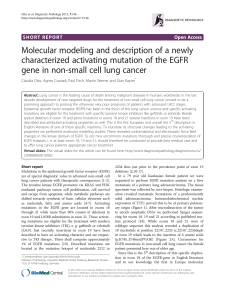
THERAPIES CIBLEES : INDICATIONS ET TOXICITES

THERAPIES CIBLEES :
INDICATIONS ET
TOXICITES
Dr Christine Gennigens
Oncologie médicale
6 Février 2016

UN PEU
D’HISTOIRE…

VOLTAIRE
1694-1778
Les mots de Voltaire
Les médecins sont des hommes qui prescrivent des médicaments
dont ils connaissent peu de choses… pour guérir des maladies
qu’ils connaissent encore moins… chez des êtres humains dont ils
ne connaissent rien.
Voltaire (1694-1778)

…La difficulté reste toujours de
soigner non seulement la
tumeur, mais surtout la
personne dans son intégralité,…
GUSTAVE ROUSSY
1874-1948
VISION HOLISTIQUE

GENERALITES
1
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
1
/
47
100%