Androgens and male physiology—The syndrome of 5 alpha

Androgens and male physiology the syndrome of 5a-reductase-2
deficiency
J. Imperato-McGinley *, Y.-S. Zhu
Division of Endocrinology, Diabetes and Metabolisms, Department of Medicine, Weill Medical College, Cornell University, 1300 York Avenue, Box 149,
Room F-260, New York, NY 10021, USA
Abstract
Dihydrotestosterone (DHT), a potent androgen, is converted from testosterone by 5a-reductase isozymes. There are two 5a-
reductase isozymes, type 1 and type 2 in humans and animals. These two isozymes have differential biochemical and molecular
features. Mutations in type 2 isozyme cause male pseudohermaphroditism, and many mutations have been reported from various
ethnic groups. The affected 46XY individuals have high normal to elevated plasma testosterone levels with decreased DHT levels
and elevated testosterone/DHT ratios. They have ambiguous external genitalia at birth so that they are believed to be girls and are
often raised as such. However, Wolffian differentiation occurs normally and they have epididymides, vas deferens and seminal
vescles. Virilization occurs at puberty frequently with a gender role change. The prostate in adulthood is small and rudimentary, and
facial and body hair is absent or decreased. Balding has not been reported. Spermatogenesis is normal if the testes are descended.
The clinical, biochemical and molecular genetic analyses of 5a-reductase-2 deficiency highlight the significance of DHT in male
sexual differentiation and male pathophysiology.
#2002 Published by Elsevier Science Ireland Ltd.
Keywords: 5a-Reductase; Androgen; Sexual development; Gender identity
1. Introduction
Male sexual development in the mammalian system
involves three sequential processes. The first step is
establishment of genetic sex by the presence of 46XY sex
chromosomes, a process completed at the time of
fertilization of the ovum. The second step is differentia-
tion of the indifferent gonad to a testis. The process of
testicular differentiation involves the SRY gene located
on the Y chromosome as well as multiple genes located
on autosomal chromosomes. The third step is transla-
tion of the gonadal sex to phenotypic sex, i.e. the
formation of internal and external genitalia. Both
testosterone and its 5areduced metabolite, DHT, play
critical roles in this process.
The importance of both androgens in male sexual
differentiation and development, and in determining
male gender identity will be discussed by reviewing the
clinical syndrome of 5a-reductase-2 deficiency.
2. 5a-Reductase isozymes
Steroid 5a-reductase isozymes are located in the
microsomes of the cell. These isozymes convert testos-
terone to DHT, a more potent androgen. They are
NADPH-dependent enzymes that reduce the double
bond at the four to five position in C
19
steroids as well as
C
21
steroids. Both testosterone and DHT bind to the
same intracellular androgen receptor, which is a member
of the nuclear steroid/thyroid hormone receptor super-
family, to regulate target gene expression (Beato, 1989).
* Corresponding author. Tel.: /1-212-746-4745; fax: /1-212-746-
8922.
E-mail address: [email protected] (J. Imperato-
McGinley).
Molecular and Cellular Endocrinology 198 (2002) 51 /59
www.elsevier.com/locate/mce
0303-7207/02/$ - see front matter #2002 Published by Elsevier Science Ireland Ltd.
PII: S 0 3 0 3 - 7 2 0 7 ( 0 2 ) 0 0 3 6 8 - 4

Although testosterone and DHT produce distinct bio-
logical responses (Wilson, 1978), they interact with the
same androgen receptor. The molecular mechanism is
unclear. However, differences in receptor binding (Wil-
bert et al., 1983) and DNA interaction (Kovacs et al.,
1984) between testosterone and DHT havebeenre-
ported.
It was theorized that multiple 5a-reductase isozymes
existed by (McGuire and Tomkins, 1960). Two different
pH optima for 5?-reductase activity in genital and
nongenital skin were detected in the 70’s (Moore and
Wilson, 1975, 1976). The major peak of 5a-reductase
activity with a narrow, acidic pH optimum of 5.5, was
found to be low in the genital skin of male pseudoher-
maphrodites with 5a-reductase deficiency. Another
broader peak of activity had a neutral to alkaline pH
(pH 7/9), which was present in both genital and
nongenital skin. This activity was found to be normal
in the genital skin of male pseudohermaphrodites with
5a-reductase deficiency. Kinetic analysis of 5a-reductase
activity in the epithelium and stroma of the prostate also
suggested different 5a-reductase activities (Bruchovsky
et al., 1988; Hudson, 1987). Studies of specific 5a-
reductase inhibitors further indicated that multiple 5a-
reductase isozymes were present in human prostate
tissues (Jenkins et al., 1992).
Two genes encoding two 5a-reductase isozymes were
eventually identified: steroid 5a-reductase type 1 (gene
symbol: SRD5A1 ) and steroid 5a-reductase type 2 (gene
symbol: SRD5A2 ), were identified, using expression
cloning, in the early 90’s (Andersson et al., 1991;
Andersson and Russell, 1990; Labrie et al., 1992).
Male pseudohermaphroditism due to 5a-reductase defi-
ciency was found to be due to mutations in the 5a-
reductase-2 gene (Andersson et al., 1991) (see Table 1).
The human 5a-reductase-2 gene, located in the short
arm of chromosome 2 band 23 has five exons and four
introns. It encodes a 254 amino acid protein which is
highly hydrophobic with a molecular weight of approxi-
mately 28.4 kDa (Andersson et al., 1991; Russell and
Wilson, 1994), and has a much higher affinity for
testosterone (apparent Km /4/50 nM) than type 1
isozyme (Km/1/5mM). The apparent Km (3/10 mM)
for the cofactor NADPH is similar for both isozymes.
The type-2 isozyme is sensitive to finasteride, a 5a-
reductase-2 inhibitor, and is expressed in external genital
tissues early in gestation (Thigpen et al., 1993a). In
adulthood, its expression in prostate, genital skin,
epididymis, seminal vesicle and liver is relatively high,
while it is quite low in other tissues. This isozyme also
appears to be expressed in the ovary and hair follicles
(Eicheler et al., 1994, 1995).
The type 2 isozyme has an acidic pH optimum in the
enzymatic assays described (Andersson et al., 1991;
Moore and Wilson, 1975; Russell and Wilson, 1994).
However, studies with transfected Chinese hamster
ovary cells suggest that the type 2 isozyme may actually
have a neutral pH optimum in its native state, and that
the acidic optimum described may actually be an artifact
of cell lysis (Thigpen et al., 1993b). Additionally,
analyses using cell lysates, permeabilized cells and intact
cells suggest that the affinity of the type 2 isozyme for
steroid substrates is higher at a neutral pH than an
acidic pH (pH 5.0), suggesting that this isozyme acts at
neutral pH in the cell (Faller et al., 1993; Thigpen et al.,
1993b).
The functional domains of the type 2 isozyme have
been deduced from in vitro mutagenesis-transfection
analysis of natural mutations of the 5a-reductase-2
isozyme in cultured mammalian cells (Can et al., 1998;
Russell and Wilson, 1994; Wigley et al., 1994), and
mutagenesis analysis of the 5a-reductase-1 isozyme
(Thigpen and Russell, 1992). Mutations affecting
NADPH binding map to the last half of the type 2
isozyme, suggesting that the carboxyl-terminal of the
isozyme appears to be a cofactor-binding domain even
though consensus adenine dinucleotide-binding se-
quences are not identified. In contrast, the type 2
isozyme mutations that affect substrate (testosterone)
binding that appear to be located at both ends of the
protein. However, due to the fact that mutations affect
either substrate or cofactor binding, but not both
(Thigpen and Russell, 1992), the amino acid determi-
nants of the substrate binding domain in the type 2
isozyme appear to be mainly located at the amino
terminal of the protein.
The 5a-reductase-1 gene is normal in male pseudo-
hermaphrodites with 5a-reductase deficiency (Anders-
son et al., 1991) and maps to the short arm of
chromosome 5 band 15. It is composed of 5 exons and
4 introns and encodes a 259 highly hydrophobic amino
acid protein with a molecular weight approximately 29.5
kDa (Russell and Wilson, 1994). It has an approxi-
mately 50% homology to the type-2 isozyme in amino
acid composition, with a broad alkaline pH optimum, a
lower substrate affinity and a lower sensitivity to
finasteride inhibition (Russell and Wilson, 1994; Zhu
et al., 1998). At birth 5a-reductase-1 is detected in the
liver and nongenital skin, and is present throughout life.
Its expression in embryonic tissues, however, is quite
low. In adulthood, it is expressed in nongenital skin,
liver and certain brain regions; whereas, its presence in
the prostate, genital skin, epididymis, seminal vesicle,
testis, adrenal and kidney is low. The physiological
function of 5a-reductase-1 is still obscure, although it
may play a role in parturition (Mahendroo et al., 1996).
In the human prostate, both 5a-reductase isozymes
are present in epithelial cells and stromal cells, while 5a-
reductase-2 is the predominant isozyme expressed in the
stromal cells (Russell and Wilson, 1994; Silver et al.,
1994; Thigpen et al., 1993a). Both isozymes are ex-
pressed in BPH and prostate cancer tissues, as well as in
J. Imperato-McGinley, Y.-S. Zhu / Molecular and Cellular Endocrinology 198 (2002) 51/5952

prostate tumor cells including LNCaP cells (Delos et al.,
1998; Guillemette et al., 1996; Negri-Cesi et al., 1998;
Smith et al., 1994).
3. Clinical presentation
The clinical syndrome of 5a-reductase deficiency was
first described, clinically and biochemically, in studies of
24 affected subjects from a large Dominican kindred
(Imperato-McGinley et al., 1974), and in two siblings
from Dallas (Walsh et al., 1974). Subsequently a large
cohort in New Guinea (Imperato-McGinley et al., 1991)
and another in Turkey were described (Akgun et al.,
1986; Can et al., 1998; Imperato-McGinley et al., 1987)
as well as many other cases worldwide [see recent review
(Zhu and Imperato-McGinley, 2002)].
We have worked with affected subjects from the
Dominican kindred for 2/3 decades; this has enabled
us to obtain important information relevant to discern-
ing the biology of testosterone and DHT in humans
(Fig. 1,Table 2).
Most affected subjects with 5a-reductase-2 deficiency
have striking ambiguity of the genitalia with a clitoral-
like phallus, severely bifid scrotum, pseudovaginal
perineoscrotal hypospadias and a rudimentary prostate
(Imperato-McGinley et al., 1974, 1979a; Imperato-
McGinley, 1992; Imperato-McGinley et al., 1992a;
Imperato-McGinley, 1996; Imperato-McGinley and Pe-
terson, 1976; Peterson et al., 1977). More masculinized
subjects have been described; they either lack a separate
vaginal opening (Imperato-McGinley et al., 1980), or
have a blind vaginal pouch which opens into the urethra
(Imperato-McGinley et al., 1979a), penile hypospadias
(Carpenter et al., 1990)oreven a penile urethra (Ng et
al., 1990).
Wolffian duct differentiation in affected subjects is
normal with seminal vesicles, vasa deferentia, epididy-
mides and ejaculatory ducts; no Mullerian structures are
present. Cryptorchidism is frequently described though
it is not invariably present with testes occasionally
located in the abdomen but usually found in the inguinal
canal or scrotum.
Male pseudohermaphrodites with 5a-reductase-2 de-
ficiency are clinical models for defining the actions of
testosterone and DHT during male sexual differentia-
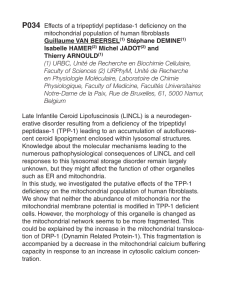
tion and development (Fig. 1). Testosterone acts on the
Wolffian ducts to cause differentiation to the vas
deferens, epididymis, and seminal vesicles. In contrast,
testosterone functions as a prehormone in the urogenital
sinus and urogenital tubercle, where it is converted to
DHT resulting in differentiation of the external genitalia
and prostate. Studies of the human fetus are supportive
of the human clinical model and demonstrate that at the
time of sexual differentiation 5a-reductase activity is
present in the urogenital sinus, urogenital tubercle and
urogenital swellings, but not in the Wolffian anlage until
sexual differentiation is completed (Siiteri and Wilson,
1974). Further supportiveevidence is provided by
animal studies in the rat by using a 5a-reductase-2
inhibitor (Imperato-McGinley et al., 1992b; Spencer et
al., 1991). However, it is puzzling that the knockout of
5a-reductase-2 or 5a-reductase-2 plus 5a-reductase-1 in
mice had normal genitalia in male offsprings (Mahen-
droo et al., 2001).
In humans, with the onset of puberty, the affected
males have increased muscle mass and deepening of the
voice (Imperato-McGinley et al., 1974). The muscula-
ture is particularly prominent in Dominican, New
Fig. 1. A diagram illustrating the roles of testosterone and DHT in male sexual differentiation in utero.
J. Imperato-McGinley, Y.-S. Zhu / Molecular and Cellular Endocrinology 198 (2002) 51/59 53

Guinean and Turkish subjects (Akgun et al., 1986; Can
et al., 1998; Imperato-McGinley et al., 1974, 1987,
1991). Affected males in these kindreds are as tall as
their unaffected siblings (Imperato-McGinley et al.,
1979a, 1981; Peterson et al., 1977). The genitalia
enlarges with growth of the phallus as well as rugation
and hyperpigmentation of the scrotum. The inguinal
testes have been observed in some subjects to descend
into the scrotum at puberty (Imperato-McGinley et al.,
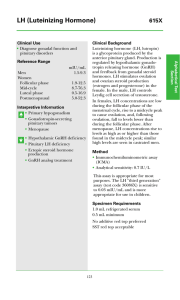
1979a, 1980, 1981). Libido is intact and affected men are
capable of erections (Fig. 2;Imperato-McGinley et al.,
1974; Imperato-McGinley and Peterson, 1979).
Although most subjects studied are generally oligo- or
azoospermic due to undescended testes; normal sperm
concentrations have been reported in subjects with
descended testes (Cai et al., 1994; Cantu et al., 1976;
Katz et al., 1997; Peterson et al., 1977). Men from the
Dominican kindred (Katz et al., 1997) and from Sweden
(Nordenskjold and Ivarsson, 1998)have been reported
to father children. These findings suggest that pubertal
events, including male sexual function and spermato-
genesis, appear to be primarily testosterone mediated
(Table 2). The other possibility is that the amount of
DHT still present is enough for spermatogenesis.
On rectal examination (Imperato-McGinley et al.,
1974) the prostate in the affected male adults is
nonpalpable (Peterson et al., 1977) and is found to be
rudimentary on transrectal ultrasound and MRI visua-
lization (Imperato-McGinley et al., 1992a). Prostatic
volumes are much smaller than those of age-matched
normal controls and are the size of prepubertal boys.
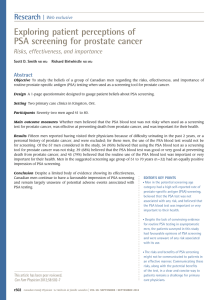
Administration of DHT can result in enlargement of the
prostate (see Fig. 3)(Imperato-McGinley et al., 1992a;
Mendonca et al., 1996). These findings provide clinical
evidence that prostate differentiation and growth is
mediated largely by DHT (see Figs. 1 and 3,Table 2).
Prostate diseases such as prostate cancer and benign
Table 2
Androgen action at puberty
Testosterone DHT
I Anabolic actions Increased facial, body hair
Muscle mass increased
Enlargement penis
Enlargement scrotum
Enlargement vocal cords
Skeletal maturation
Growth spurt
Epiphyseal closure
II Spermatogenesis Scalp hair recession
III Male sex drive, performance Prostate enlargement
IV Pituitary-gonadal feedback Pituitary-gonadal feedback
Fig. 2. A representative recording of nocturnal penile tumescence and
rigidity from penile base and tip in a 21-year-old subject with 5a-
reductase-2 deficiency. It shows the presence of sleep-related erections.
Table 1
Comparison of human 5a-reductase isozymes
Type 1 Type 2
Gene structure 5 exons, 4 introns 5 exons, 4 introns
Gene, chromosome location SRD5A1 , 5p15 SRD5A2 , 2p23
Size 259 amino acids, Mr/29 462 254 amino acids, Mr/28 398
Tissue distribution Liver, nongenital skin, prostate, brain,
ovary, testis
Prostate, epididymis, seminal vesicle, genital skin, liver, uterus, breast, hair
follicle, placenta, testis
Prostate level Low High
Activity in 5a-reductase de-
ficiency
Normal Mutated
J. Imperato-McGinley, Y.-S. Zhu / Molecular and Cellular Endocrinology 198 (2002) 51/5954

prostate hyperplasia have not been reported in affected
males.
The facial and body hair is decreased, and male
pattern baldness has never been observed in genetic
males with this condition (Akgun et al., 1986; Imperato-
McGinley et al., 1974, 1991).
Sebum production is dependent on androgen action.
No demonstrable sebum is produced in 46XY subjects
with complete androgen insensitivity due to androgen
receptor mutation confirming its dependency (Imperato-
McGinley et al., 1993). However, the affected subjects
with 5a-reductase-2 deficiency have normal sebum
production, suggesting that sebum production is not
regulated by 5a-reductase-2 isozyme (Imperato-McGin-
ley et al., 1993).
Homozygous females with a 5a-reductase-2 gene
mutation and decreased plasma DHT appear to have
decreased body hair and delayed menarche but normal
to enhanced fertility (Katz et al., 1995; Milewich et al.,
1995). Since 5a-reductase-2 is expressed in the ovary
(Eicheler et al., 1994), and our unpublished data] a
defect in this isozyme may decrease DHT production in
the ovary, resulting in an elevated estrogen to DHT
ratio, thereby, facilitating ovulation and infertility (Katz
et al., 1995).
4. Biochemical features of 5a-reductase-2 deficiency
Over the years, the biochemical features of this
syndrome have been well defined (see recent reviews
Imperato-McGinley, 1996; Zhu et al., 1998). These
include: (a) normal to elevated levels of plasma testos-
terone; (b) decreased levels of plasma DHT; (c) an
increased testosterone to DHT ratio at baseline and/or
following hCG stimulation; (d) decreased conversion of
testosterone to dihydrotestosterone (DHT) in vivo; (e)
normal metabolic clearance rates of testosterone and
DHT; (f) decreased production of urinary 5a-reduced
androgen metabolites with increased 5b/5aurinary
metabolite ratios; (g) decreased plasma and urinary
3a-androstanediol glucuronide, a major metabolite of
DHT; (h) a global defect in steroid 5a-reduction as
demonstrated by decreased urinary 5a-reduced metabo-
lites of both C
21
steroids and C
19
steroids other than
testosterone, i.e. cortisol, corticosterone, 11b-hydroxy-
androstenedione and androstenedione; (i) increased
plasma levels of LH and an increased LH pulse
amplitude with a normal LH frequency (Canovatchel
et al., 1994); (j) plasma FSH levels may be elevated.
5. Defects in the 5a-reductase-2 gene
The first identified genetic defect of 5a-reductase
deficiency was carried out in male pseudohermaphro-
dites from our New Guinean kindred (Andersson et al.,
1991). To date, over 33 mutations in the 5a-reductase-2
gene (Wilson et al., 1993; Nordenskjold et al., 1998;
Vilchis et al., 2000; Zhu et al., 1998 and our unpublished
data) have been identified, including mutations in the
three largest kindreds of male pseudohermaphrodites
with 5a-reductase-2 deficiency in the world */the Do-
minican, New Guinean and Turkish kindreds. A dele-
tion of more than 20 kb in the 5a-reductase-2 gene was
found in the subjects from New Guinean kindred by
Southern blot analysis (Andersson et al., 1991). In the
Dominican kindred, a missense mutation was found in
exon 5 of the 5a-reductase-2 gene, substituting thymi-
dine for cytosine and resulting in a substitution of the
non-polar amino acid tryptophan for the basic, polar
amino acid arginine at position 246 (R246W) of the
isozyme (Cai et al., 1996; Thigpen et al., 1992a). The
mutated isozyme has a decreased binding to the
cofactor, NADPH, an altered pH optimum and a
dramatic loss of enzymatic activity (Thigpen et al.,
Fig. 3. Representative sonograms showing the enlargement of prostate in a 5a-reductase-2 deficient patient pre DHT treatment (A) and post 2%
DHT cream (B) applied to the genital area for approximately 3 months. Note the crosses at the outer edges of the prostate.
J. Imperato-McGinley, Y.-S. Zhu / Molecular and Cellular Endocrinology 198 (2002) 51/59 55
 6
7
8
9
6
7
8
9
1
/
9
100%