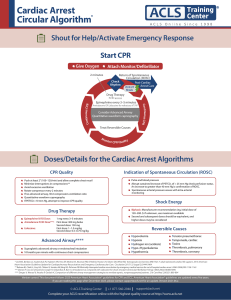
Factors in Pediatric ECPR Initiation: International Survey
Telechargé par
Duy-Anh Nguyen

Copyright © ASAIO 2021
1
ASAIO Journal 2021 Pediatric Circulatory Support
Factors Associated With Initiation of Extracorporeal
Cardiopulmonary Resuscitation in the Pediatric Population:
An International Survey
DUY-ANH NGUYEN ,*† AURÉLIE DE MUL ,†‡ APARNA U. HOSKOTE ,§ PAOLA COGO ,¶ EDUARDO M. DA CRUZ,∥
SIMON ERICKSON,# JAVIER J. LASA,** RAVI R. THIAGARAJAN,†† MELANIA M. BEMBEA ,‡‡ AND OLIVER KARAM ,§§
on behalf of PALISI, ESPNIC, ANZICS PSG
Although extracorporeal cardiopulmonary resuscitation
(ECPR) is increasingly utilized in the pediatric critical care
environment, our understanding regarding pediatric candi-
dacy for ECPR remains unknown. Our objective is to explore
current practice and indications for pediatric ECPR. Scenario-
based, self-administered, online survey, evaluating clinical
determinants that may impact pediatric ECPR initiation with
respect to four scenarios: postoperative cardiac surgery, car-
diac failure secondary to myocarditis, septic shock, and chronic
respiratory failure in a former preterm child. Responders are
pediatric critical care physicians from four societies. 249
physicians, mostly from North America, answered the survey.
In cardiac scenarios, 40% of the responders would initiate
ECPR, irrespective of CPR duration, compared with less than
20% in noncardiac scenarios. Nearly 33% of responders
would consider ECPR if CPR duration was less than 60 min-
utes in noncardiac scenarios. Factors strongly decreasing the
likelihood to initiate ECPR were out-of-hospital unwitnessed
cardiac arrest and blood pH <6.60. Additional factors reduc-
ing this likelihood were multiple organ failure, pre-existing
neurologic delay, >10 doses of adrenaline, poor CPR quality,
and lactate >18 mmol/l. Pediatric intensive care unit loca-
tion for cardiac arrest, good CPR quality, 24/7 in-house extra-
corporeal membrane oxygenation (ECMO) team moderately
increase the likelihood of initiating ECPR. This international
survey of pediatric ECPR initiation practices reveals signifi-
cant differences regarding ECPR candidacy based on patient
category, location of arrest, duration of CPR, witness status,
and last blood pH. Further research identifying prognostic
factors measurable before ECMO initiation should help define
the optimal ECPR initiation strategy. ASAIO Journal 2021;
XX;1–1
Key Words: cardiac arrest, extracorporeal membrane oxygen-
ation, cardiopulmonary resuscitation, heart failure, respira-
tory insufficiency, surveys and questionnaires, intensive care
units, pediatric
Extracorporeal cardiopulmonary resuscitation (ECPR) pro-
vides cardiac output in situations of refractory cardiac arrest
when conventional CPR fails to restore spontaneous circu-
lation. Extracorporeal cardiopulmonary resuscitation has
become a substantial modality of extracorporeal life support,
accounting for 25% of all pediatric extracorporeal membrane
oxygenation (ECMO) runs reported to the Extracorporeal Life
Support Organization (ELSO) between 1989 to 2016,1 and has
been triggered in 27.2% of all cardiac arrest events across the
Pediatric Cardiac Critical Care Consortium’s cardiac intensive
care units (CICU) between 2014 and 2016.2 The number of
ELSO-reported ECPR cases has increased by 35% for neonatal
ECPR and 67% for pediatric ECPR in 2015 when compared
with 2009.1,3 In the last two decades, the overall survival rate to
hospital discharge following neonatal and pediatric ECPR has
been stable at around 45%.3,4 In a retrospective study by Lasa
et al.5 analyzing 3,756 in-hospital pediatric cardiac arrest
events requiring more than 10 minutes of CPR, survival to
discharge, as well as survival with favorable neurologic out-
come, were greater for ECPR patients versus conventional CPR
patients.
Currently, the international guidelines only support ECPR for
children with cardiac disease. Similar to the 2020 International
Consensus on Cardiopulmonary Resuscitation and Emergency
From the *Pediatric Cardiology Unit, Department of Women-
Children-Teenagers, Geneva University Hospitals, Geneva,
Switzerland; †Pediatric Intensive Care Unit, Department of Women-
Children-Teenagers, Geneva University Hospitals, Geneva,
Switzerland; ‡Pediatric Nephrology Unit, Department of Women-
Children-Teenagers, Geneva University Hospitals, Geneva,
Switzerland; §Cardiac Intensive Care Unit, Heart and Lung Directorate,
Great Ormond Street Hospital National Health Service Foundation
Trust, London, United Kingdom; ¶Department of Medicine, University
Hospital of S Maria della Misericordia, University of Udine, Udine,
Italy; ∥Department of Pediatrics, Heart Institute, Pediatric Cardiac
Critical Care Section, Children’s Hospital Colorado, University of
Colorado Denver School of Medicine, Aurora, Colorado; #Department
of Paediatric Critical Care, Perth Children’s Hospital, Perth, Western
Australia; **Sections of Critical Care Medicine and Cardiology,
Department of Pediatrics, Texas Children’s Hospital, Houston, Texas;
††Division of Cardiac Critical Care, Department of Cardiology,
Boston Children’s Hospital, Boston, Massachusetts; ‡‡Department of
Anesthesiology and Critical Care Medicine, Johns Hopkins University,
Baltimore, Maryland; and §§Division of Pediatric Critical Care
Medicine, Department of Pediatrics,Children’s Hospital of Richmond
at Virginia Commonwealth University, Richmond, Virginia.
Submitted for consideration February 2021; accepted for publica-
tion in revised form April 2021.
Disclosure: The authors have no conflicts of interest to report.
This study was supported by the Clinical and Translational Science
Award No. UL1TR000058 from the National Center for Advancing
Translational Sciences (for access to Research Electronic Data Capture).
M.M.B.’s institution received funding from the National Institutes of
Health/National Institute of Neurological Disorders and Stroke.
Supplemental digital content is available for this article. Direct URL
citations appear in the printed text, and links to the digital files are
provided in the HTML and PDF versions of this article on the journal’s
Web site (www.asaiojournal.com).
Correspondence: Oliver Karam, Division of Pediatric Critical Care
Medicine, Children’s Hospital of Richmond at Virginia Commonwealth
University, 1250 E Marshall Street, Richmond, VA 23298. Email: oliver.
Copyright © ASAIO 2021
DOI: 10.1097/MAT.0000000000001495
LWW

Copyright © ASAIO 2021
NGUYEN ET AL.
2
Cardiovascular Care Science With Treatment Recommendations
(CoSTR),6 the 2020 American Heart Association (AHA)
Guidelines for Cardiopulmonary Resuscitation and Emergency
Cardiovascular Care states “ECPR may be considered for
pediatric patients with cardiac diagnoses who have in-hospi-
tal location of cardiac arrest (IHCA) in settings with existing
ECMO protocols, expertise, and equipment.”7
However, despite potentially promising results, this complex
therapy is associated with important morbidity and mortality, as
well as substantial financial and staffing resources. Therefore,
it is important to identify patients who are likely to benefit the
most from it. Previous studies have shown significant variabil-
ity in ECPR practice regarding timing of ECMO initiation, risk
profile for various laboratory results.8,9 Furthermore, indica-
tions for ECPR in noncardiac disease or out-of-hospital cardiac
arrests (OHCA) are not currently known. In a linkage study
between ELSO and the American Heart Association Get With
The Guidelines Resuscitation Registry—two large U.S. multi-
center registries—79% of all the reported 593 ECPR cases from
2000 to 2014 were classified as surgical cardiac or medical
cardiac.10 Thus, over 15 years of North American reporting,
only 125 children contributed to the noncardiac ECPR data.
The objective of this study is to describe the current stated
practice regarding pediatric ECPR initiation, based on various
clinical scenarios, duration of CPR, laboratory values, and
ECMO infrastructure.
Materials and Methods
Study Design
This web-based survey used a scenario-based questionnaire,
which was approved for distribution by ELSO and endorsed by
the following medical societies: Pediatric Acute Lung Injury
and Sepsis Investigators (PALISI) Network, European Society
of Paediatric and Neonatal Intensive Care (ESPNIC), and
Australian and New Zealand Intensive Care Society Paediatric
Study Group (ANZICS PSG).
Study Population
Targeted respondents were pediatric critical care physicians
(excluding those in training), who were members of at least
one of the previously cited societies: ELSO, PALISI, ESPNIC,
and ANZICS PSG.
Development of the Questionnaire
Twenty clinical determinants potentially affecting initiation
of ECPR were first identified through consultation with eight
experts in pediatric critical care and ECMO, all members of the
study steering committee and from the four societies. Second,
these experts discussed the 14 determinants that would be
retained for the final survey.
Four different areas were recognized and addressed in the sur-
vey: acute cardiac failure, chronic cardiac failure, acute noncar-
diac hemodynamic failure, and chronic respiratory failure. The
clinical scenarios, described in Table1, were cardiac arrest after
cardiac surgery, after chronic cardiac failure secondary to myo-
carditis, after septic shock, and after worsening chronic respira-
tory failure secondary to bronchopulmonary dysplasia.
Within each of the four scenarios, respondents were asked
what duration of CPR would disqualify the use of ECPR.
Extracorporeal cardiopulmonary resuscitation was defined as
the application of rapid-deployment venoarterial ECMO, that
is, cannulation and initiation of flow, to provide circulatory sup-
port in patients in whom conventional CPR is unsuccessful in
achieving sustained return of spontaneous circulation.11 Seven
responses were possible to the question “what duration of CPR
would disqualify the use of ECPR”: the respondent would initi-
ate ECPR whatever the duration of CPR; the respondent would
initiate ECPR only if the duration of CPR were ≤5 minutes;
≤10 minutes; ≤20 minutes; ≤30 minutes; ≤60 minutes; or the
respondent would not initiate ECPR, regardless of the duration
of CPR.
Thereafter, we asked the effect of the following clinical
determinants on the likelihood to initiate ECPR or not, using a
9-point Likert scale (from 1, strongly decreases the likelihood
to initiate ECMO, to 9, strongly increases the likelihood to initi-
ate ECMO).
The clinical determinants were divided into three subcatego-
ries: 1) Cardiac arrest and CPR-related determinants: duration of
CPR; location of cardiac arrest (IHCA versus OHCA); witnessed
cardiac arrest or not; presence or absence of a witness/bystander
who provides CPR; IHCA (pediatric ward versus intensive care
unit [ICU]); quality of CPR (good versus poor, as evaluated by
the clinician, according to the frequency of interruptions or the
depth and speed of chest compressions or physiologic markers
such as end-tidal carbon dioxide and invasive diastolic blood
pressure); last blood gas pH; last blood lactate; and number of
adrenaline (epinephrine) doses; 2) Patient-related determinants:
age of the patient; pre-existing condition unrelated to the car-
diac arrest (severe neurodevelopmental delay, biventricular
versus single ventricle postcardiac surgery physiology (for the
scenario involving a postcardiac surgery arrest), one other organ
failure besides cardiovascular failure or multiple organ failure);
and 3) Hospital-level determinants: in-house ECMO team 24/7
and an existing heart transplantation program.
At the end of the survey, respondents were asked, in free
text, what other variables they would consider before placing
a patient in cardiac arrest on ECMO.
Respondents’ demographics were the last questions of the
survey. The full survey is available as Supplemental Digital
Content 1, http://links.lww.com/ASAIO/A661.
Table 1. The Four Cardiac Arrest Scenarios
Acute
cardiac
diagnosis
1-year-old patient, who just underwent heart
surgery, develops a refractory cardiac arrest in
the PICU. There is no bleeding involved.
Chronic
cardiac
diagnosis
1-year-old patient, admitted to PICU for cardiac fail-
ure secondary to viral myocarditis, develops
a refractory cardiac arrest.
Noncardiac
acute
diagnoses
1-year-old patient, admitted to the ER for refractory
septic shock, develops subsequent refractory
cardiopulmonary arrest.
Noncardiac
chronic
diagnosis
1-year-old patient, with a history of prematurity
and chronic respiratory failure secondary to
bronchopulmonary dysplasia, admitted to the
ER for refractory cardiopulmonary arrest.
Refractory cardiac arrest was dened as a situation where
conventional cardiopulmonary resuscitation is unsuccessful in
achieving sustained return of spontaneous circulation.
ER, emergency room; PICU, pediatric intensive care unit.

Copyright © ASAIO 2021
PEDIATRIC ECPR: AN INTERNATIONAL SURVEY 3
Questionnaire Formatting and Pretesting
The survey instrument was developed in English and format-
ted using Research Electronic Data Capture hosted at Virginia
Commonwealth University (Vanderbilt University, Nashville,
TN).12
The final questionnaire was validated with the following
strategy. First, 10 critical care physicians (separate from the
steering committee), who have practiced in a pediatric criti-
cal care unit for at least 5 years and each worked in a differ-
ent unit, pretested the survey for relevance, completeness, and
accuracy. The survey was then adapted accordingly.
As a second step, 10 other critical care physicians (also
separate from the steering committee), who have practiced
in a pediatric critical care unit for at least 5 years and each
worked in a different unit, then answered the survey twice,
within a 2-week interval, to test for intrarater reproducibil-
ity. Concordance rate and kappa coefficients were used to
describe reproducibility. Overall, the intrarater concordance
for the answers given 2 weeks apart was 96% (95% confi-
dence interval [CI], 90–99). The same pilot responders also
rated the survey for relevance, completeness, and accuracy
by using a 7-point Likert scale ranging from 1 (complete dis-
agreement) to 7 (complete agreement). The median values
for relevance, completeness, and accuracy were 7, 6, and 6,
respectively.
Ethical Consideration
As this study was about physician opinions and did
not involve patients, Swiss regulations did not consider
it to be research on human subjects. Therefore, Geneva’s
institutional review board (Commission Cantonale
d’Ethique de la Recherche) waived the need to review this
survey.
The participants were considered to have consented to the
survey when they submitted their results online. The data col-
lected were anonymous, and only aggregated demographic
data have been presented in the results, such as gender, coun-
try, and years of clinical experience (number of years since
graduating from fellowship or training).
Administration of the Questionnaire
The survey was carried out according to the recommenda-
tions made by Burns et al.13 After getting official approval by
each society, a link to the survey was sent to the members on
their respective mailing list, between December 2019 and
February 2020. A reminder was sent 2 weeks later, followed by
a third mailing 1 month after the first.
Statistical Analysis
Because the invitation to participate in the survey was sent
directly by the different societies, to ensure anonymity and to
conform to the societies’ guidelines, we were not able to deter-
mine if some recipients received the survey link more than
once nor were we able to distinguish which responses came
from specific institutions or if multiple representatives from
the same institution responded to the survey. Additionally, we
were not able to target our invitation emails only to physicians.
For example, the ELSO database does not allow ascertaining if
the ECMO coordinator is a physician. Therefore, as we were
not able to calculate the denominator, we will not be able to
report a response rate.
Responses are reported as counts and percentage with 95%
CI, or as medians and interquartile range (IQR), as appropri-
ate. We had planned a priori to categorize the answers to the
Likert scales into “decreased likelihood,” “undetermined effect
on likelihood,” and “increased likelihood” for Likert points of
1–4, 5, and 6–9, respectively. Within each of these categories,
we considered a strong and moderate effect on likelihood for
a rate of responders of 80–100% and 60–80%, respectively.
Nonparametric statistics (Mann-Whitney U test for continuous
Table 2. Work Environment and ECMO Equipment
Variables N %
Region
North America 125 82
Central or South America 0 0
Europe 17 11
Asia 0 0
Africa 0 0
Australia and New Zealand 11 7
Unanswered 98
ICU category
General pediatric patients (PICU) 134 88
Cardiac surgery patients (CICU) 70 46
Neonatal patients (NICU) 7 6
Unanswered 98
Number of ECMO runs/year
Median and IQR 15 (8 to 30)
Unanswered 98
Availability of ECPR
Yes 111 78
No 32 22
Unanswered 108
ECPR 24/7 availability
Yes 100 90
No 11 10
Unanswered 140
ECPR ECMO circuit priming
Primed ECPR circuit 83 78
No primed ECPR circuit 24 22
Unanswered 144
Cardiac catheterization 24/7 availability
Yes 117 86
No 23 16
Unanswered 111
Cardiac imaging 24/7 availability
Yes 130 92
No 12 8
Unanswered 109
Neurology service 24/7 availability
Yes 133 94
No 9 6
Unanswered 109
Type of ECMO priming
Blood prime 16 11
Clear prime 20 14
One or the other, depending on age 10 73
Other 32 1
Unanswered 110
Type of ECMO pump
Centrifugal pump 133 94
Roller head pump 15 11
Unanswered 110
Values are described as either median (IQR) or number (%).
CICU, cardiac intensive care unit; ECMO, extracorporeal
membrane oxygenation; ECPR, extracorporeal cardiopulmonary
resuscitation; ICU, intensive care unit; IQR, interquartile range;
NICU, neonatal intensive care unit; PICU, pediatric intensive care
unit.

Copyright © ASAIO 2021
NGUYEN ET AL.
4
variables, Fisher exact test for ordinal or binary variables) were
applied when comparing groups (large versus small ECMO
centers, North America versus rest of the world, or senior ver-
sus junior physicians, defined as more than 10 years of profes-
sional experience).
Proportion of missing data was reported in the results, but
no imputations were made as it was impossible to evaluate if
missing data were random or associated with the scenarios or
the respondents.
Differences were considered statistically significant when a
two-sided α level was <0.05. No adjustments were made for
multiple comparisons, as the different questions are not inde-
pendent and as this would increase the risk of type II errors. All
statistical analyses were performed with SPSS version 26 for
Mac (SPSS, Chicago, IL).
Results
Respondents’ Demographics
Among the 249 respondents, 61% (153/249) provided
demographic data and the majority were from North America
(82%, 125/153). The median age was 44 years (IQR, 35–52),
50% (76/153) had more than 10 years of experience. Ninety-
nine percent (152/154) were pediatric critical care physi-
cians, the other two respondents were a pediatric cardiologist
and pediatric cardiothoracic surgeon. Eighty-eight percent
(134/153) worked in a pediatric intensive care unit (PICU) and
46% (70/153) in CICU (categories were not mutually exclu-
sive). Table 2 summarizes work environment characteristics
and ECMO equipment.
Effects of Scenarios on Cardiopulmonary Resuscitation Duration
Disqualifying the Use of Extracorporeal Cardiopulmonary
Resuscitation
As shown in Figure1, more than 99% of respondents would
consider ECPR, regardless of the scenario and the CPR duration.
Few providers would not consider ECPR regardless of the duration
of CPR: 0.5% for postoperative cardiac arrest, 0.6% for arrest sec-
ondary to viral myocarditis, 1.5% for arrest in septic shock, and
0.9% for arrest secondary to chronic respiratory failure, p = 0.47.
However, the effect of the duration of CPR varied accord-
ing to the scenarios. More than a third of the responders
would initiate ECPR, irrespective of CPR duration (i.e., with
no time-limit), in scenarios involving cardiac patients (44%
for postoperative cardiac arrest, 36% for arrest secondary to
viral myocarditis), compared with less than 20% in noncar-
diac scenarios (20% for arrest in septic shock and 16% for
arrest secondary to chronic respiratory failure, p < 0.001).
None of the respondents’ demographic variables were
associated with the likelihood to initiate versus not initiate
ECPR regardless of the duration of CPR (gender, p = 0.60; age,
p = 0.86; region, p = 0.26; cardiology versus critical primary
training, p = 0.15; years since end of training, p = 0.40; offer-
ing ECPR at their center, p = 0.13; and number of ECMO runs
per year, p = 0.31). Furthermore, missing demographic infor-
mation was not associated with the duration of CPR (p = 0.52).
Effects of the Clinical Determinants
As shown in Table 3, factors strongly decreasing the like-
lihood to initiate ECPR, regardless of the scenario, were
Figure 1. Histogram of the responses to the question “What duration of CPR would disqualify the use of ECPR.” “Never initiate ECPR”
means the respondent would not initiate ECPR regardless of duration of CPR; “only if <5 min” means the respondent would initiate ECPR
only if the duration of CPR was less than 5 minutes; and “always initiate ECPR” means the respondent would initiate ECPR whatever the
duration of CPR. The four scenarios are a cardiac arrest after cardiac surgery (scenario 1, in black); cardiac arrest secondary to viral myocar-
ditis (scenario 2, in dark gray); cardiac arrest secondary to septic shock (scenario 3, in light gray); and cardiac arrest in a patient with chronic
respiratory failure secondary to bronchopulmonary dysplasia (scenario 4, in white). CPR, cardiopulmonary resuscitation; ECPR, extracorpo-
real cardiopulmonary resuscitation.

Copyright © ASAIO 2021
PEDIATRIC ECPR: AN INTERNATIONAL SURVEY 5
out-of-hospital unwitnessed cardiac arrest (assessed only in
noncardiac scenarios) and blood pH <6.60. Factors moder-
ately decreasing the likelihood of initiating ECPR were multi-
ple organ failure, pre-existing neurologic delay, administration
of >10 doses of adrenaline, poor CPR quality, lactate >18
mmol/L, and blood pH between 6.61 and 6.84.
Discussion
This survey suggests a high level of heterogeneity in ECPR ini-
tiation practice relating to various CPR durations and potential
factors impacting the physician’s decision. Only about 1% of
responders would never initiate ECPR, regardless of the scenario
and the duration. More than a third of the responders would ini-
tiate ECPR irrespective of CPR duration in scenarios involving
cardiac patients as compared with less than 20% in noncardiac
scenarios. On the other hand, more than 30% of the responders
would still consider ECPR if CPR duration was up to 60 minutes in
noncardiac scenarios. Factors strongly decreasing the likelihood
to initiate ECPR, regardless of the scenario, were out-of-hospital
unwitnessed cardiac arrest and blood pH <6.60. There was more
heterogeneity in the impact of multiple organ failure, pre-existing
neurologic delay, doses of adrenaline, CPR quality, and lactate.
Compliance With Current Guidelines
This survey allows us to compare stated practice with current
⇣⇣. Our results suggest more than 99% of the responders would
consider ECPR, including in noncardiac patients. However,
international guidelines (CoSTR) and AHA only support ECPR
deployment for IHCA in patients with cardiac diagnoses,6,7,14
based on different pathophysiology (e.g., noncardiac patients
having more hypoxic cardiac arrests compared to those with
primary cardiac disease) leading perhaps to better outcomes,
and lack of data.4,10
Additionally, our survey seems to indicate that 10% of the
responders do not believe that OHCA affects their decision to
initiate ECPR. Although the current recommendations do not
support OHCA ECPR, pediatric studies are scarce as OHCA
ECPR represents only 2% of ECPR cases reported to ELSO.3
This lack of adherence to guidelines could be due to the low
quality of current evidence.
Relevance of Cardiopulmonary Resuscitation
Duration on Scenario-Based Decision
Our survey shows more than a third of the responders would
initiate ECPR, irrespective of CPR duration in scenarios involving
cardiac patients; and, in noncardiac scenarios, 30% of respond-
ers would still consider initiating ECPR for CPR duration between
30 and 60 minutes. These data are probably explained by several
studies reporting survival with good neurologic outcomes even in
cases of CPR duration up to 120 minutes, especially in cardiac
patients. However, there are conflicting data on ECPR duration
and outcomes. Several pediatric and adult studies have shown an
association between longer duration of resuscitation before ECPR
initiation and decreased survival.15 In a retrospective study includ-
ing 593 children from two multicenter databases, the odds of death
increased by 4% for every 5-minute increase in time from onset of
resuscitation.10 In a retrospective study from Switzerland, we also
found an association between longer pre-ECMO resuscitation and
Table 3. Effects of the Clinical Determinants on the Likelihood
to Increase, Having Undetermined Effect or Decrease the
Initiation of Extracorporeal Cardiopulmonary Resuscitation
Clinical Determinants Scenario 1 Scenario 2 Scenario 3 Scenario 4
Localization
Pediatric ward = =
PICU ↑⇡
CPR quality*
Good ⇧↑↑⇡
Poor ↓⇣↓ ↓
Last pH
>7 ⇡− − =
6.85–7 = = = =
6.61–6.84 ⇣ ⇣ ↓⇣
<6.60 ⇩ ⇩ ↓⇩
Last lactate
<8 = = = =
8–13.9 = = = =
14–17.9 − − ⇣ ⇣
>18 ⇣↓ ↓ ↓
Epinephrine doses
1–3 = = = =
4–6 ≡ ≡ = =
7–9 − = − −
>10 ⇣ ⇣ ↓ ↓
Age
<7 d ≡ ≡ =
8 d–364 d ≡≡≡
<1 y ≡
1–5 y ≡ ≡ ≡ ≡
6–18 y ≡ ≡ ≡ ≡
Cardiac physiology
Biventricular =
Single ventricle =
Developmental delay
Yes ↓⇩↓ ↓
No ⇡−/⇡ tie − −
Organ failure
No ↑⇡ ⇡ −
One other† = = = =
Multiple ↓ ↓ ↓ ↓
In-house ECMO team
Yes ↑ ↑ ⇡↑
No = = − −
Heart transplant program
Yes = = ≡
No ≡ ≡ ≡
IHCA vs. OHCA
IHCA ↑ ↑
OHCA ⇩ ⇩
Witnessed CA
Yes ↑ ↑
No ⇩ ⇩
Witnessed/bystander providing CPR
Yes − −
No ⇩ ⇩
Zones left blank are questions that were not asked (such as
the effect of OHCA for a postsurgical cardiac arrest in the PICU).
⇡/↑/⇧: mildly/moderately/strongly increased likelihood to initiate
ECPR. −/=/≡: mild/moderate/strong undetermined effect on likeli-
hood to initiate ECPR. ⇣/↓/⇩: mildly/moderately/strongly decreased
likelihood to initiate ECPR.
*CPR quality is evaluated by the clinician, according to the fre-
quency of interruptions or the depth and speed of chest compres-
sions or physiologic markers such as end-tidal carbon dioxide and
invasive diastolic blood pressure.
†One other organ failure besides cardiovascular failure.
CA, cardiac arrest; CPR, cardiopulmonary resuscitation; ECMO,
extracorporeal membrane oxygenation; ECPR, extracorporeal car-
diopulmonary resuscitation; IHCA, in-hospital location of cardiac
arrest; OHCA, out-of-hospital location of cardiac arrest; PICU, pedi-
atric intensive care unit.
 6
6
1
/
6
100%