Salivary Gland Tumors: WHO Classification Update & Challenges
Telechargé par
dienemamadou9.3

Salivary gland tumours:
diagnostic challenges and
an update on the latest
WHO classification
Paul M Speight
A William Barrett
Abstract
Salivary gland tumours are one of the most difficult areas of diagnostic
pathology, with significant morphological diversity and many overlap-
ping features. The latest WHO classification has attempted to simplify
the classification but there are still more than 30 tumours for the
pathologist to grapple with. These include two new entities esecre-
tory carcinoma and sclerosing polycystic adenosis eand a number
of name changes. Most controversial is the removal of “low grade”
from polymorphous low-grade adenocarcinoma and the inclusion of
intraductal carcinoma as a unifying entity. There are also more
nuanced changes in categorisation or terminology that may influence
the way a diagnostic report is written. Despite advances in immunohis-
tochemistry and molecular pathology, the WHO still use histomorphol-
ogy as the primary basis for classification. However, morphological
similarities can make diagnosis difficult without the assistance of ancil-
lary techniques. In this short review we describe these changes in the
latest WHO classification, discuss particular areas of diagnostic diffi-
culty, and suggest some useful antibodies that can be used to assist
diagnosis.
Keywords classification; diagnostic difficulties; immunohistochem-
istry; salivary gland tumours; WHO classification
Introduction and overview
Primary epithelial salivary gland tumours (SGT) are a morpho-
logically diverse group of neoplasms, which may present
considerable diagnostic challenges to the pathologist, and man-
agement conundra to surgeons and oncologists. SGT are rare,
with only about 720 cases per year in the United Kingdom.
1
The
overall incidence of benign and malignant tumours is less than 5
per 100,000 head of population per year. Since about 80% of all
tumours are benign it can be appreciated that salivary gland
malignancies are very rare with reported incidences of only 1.2
e1.3 cases per 100,000 and representing only around 3% of all
cancers of the head and neck.
1,2
As a general rule patients are
over the age of 40 with males and females equally affected.
However, it is important to note that some of the more common
tumours, especially pleomorphic adenoma (PA), show a pre-
dominance for females with a M:F ratio of about 1:1.4.
3
Around 80% of SGT are benign and 65% of these are PA
which are by far the most common of all SGT, comprising about
55% of major gland lesions and 50% of minor gland lesions.
3,4
Tumours in the parotid gland account for approximately 70%
of SGT, the submandibular gland accounts for around 10% and
the sublingual gland less than 1%, thus the minor glands are
affected by about 20%. Although tumours are less common in
the minor glands about 50% are malignant, compared to only
about 20% in the major glands. Of note, tumours in the sublin-
gual gland are almost always malignant. Of the 70% of all tu-
mours encountered in the parotid gland, 50e60% are PA, 20
e30% are Warthin tumours and about 10% are mucoepidermoid
carcinomas (MEC).
2e4
There is a dauntingly extensive literature on this topic, but for
the diagnostic pathologist there are a number of excellent current
histopathology textbooks
5,6
which, as well as the latest AFIP
fascicle
7
and current WHO classification,
8
may provide succinct
guidance.
In this article we aim to update our previous review
9
of the
main changes in the latest WHO classification of salivary gland
tumours and address some areas of interest, dispute and
difficulty.
Changes in the classification of salivary gland tumours
In 1952, the World Health Organization (WHO) initiated a pro-
gramme to produce an internationally acceptable classification
system for all human tumours. The process has been reviewed by
Sobin,
10
but the overall aim was to produce classifications that
would use a uniform nomenclature to facilitate global commu-
nication. Number 7 in the series was published in 1972 and was
the first edition of the WHO classification of salivary gland tu-
mours.
11
This first classification listed only 10 primary epithelial
SGT using terminology which, with three exceptions, current
pathologists would not recognize. By the time of the second
edition in 1991
12
the number of entities had risen significantly to
39. These classifications were based almost exclusively on his-
tomorphology and were essentially a simple list of lesions or-
dered by frequency of occurrence. Such a classification system
has been criticized, especially by surgical oncologists, for being
too complicated and for a lack of precision or applicability to
modern oncological practice. In a previous review, we discussed
at length the benefits or otherwise of “lumping” or “splitting”
SGT
4
and suggested that these comprehensive classifications had
developed because of the wide morphological diversity of the
tumours, and were needed to ensure accurate diagnosis and
correct categorisation which in turn would guide treatment. We
believe that this is still the case, and indeed subsequent editions
of the WHO classification have maintained this approach. In the
2005 classification
13
the number of entities remained virtually
stable at 37, and in the latest (2017) classification has been
slightly reduced to 33.
8
The major changes in the classification are summarized in
Table 1 and are discussed below. The reason for the reduction
Paul M Speight BDS PhD FDSRCPS FDSRCS (Eng) FDSRCS (Ed) FRCPath,
Professor of Oral and Maxillofacial Pathology, School of Clinical
Dentistry, University of Sheffield, Sheffield, UK. Conflicts of interest:
none declared.
A William Barrett BDS MSc PhD FDSRCS (Ed) FDSRCS (Eng) FRCPath,
Consultant Histopathologist, Department of Histopathology, Queen
Victoria Hospital, East Grinstead, UK. Conflicts of interest: none
declared.
MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY
DIAGNOSTIC HISTOPATHOLOGY 26:4 147
Ó2020 The Authors. Published by Elsevier Ltd. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).

was explained by El-Naggar in the introduction to the 2017 WHO
classification.
8
There was an overall desire to make the classifi-
cation less complex and more streamlined. Therefore, some
particularly rare malignant entities were grouped together as
“adenocarcinoma NOS” and the two variants of ductal papilloma
(intraductal papilloma, inverted ductal papilloma) were merged.
Despite several candidates, only two new entities were included,
as they had thoroughly documented novel phenotypes and had
become universally recognized. Also, a major principle of the
WHO’s international approach has been maintained ethat
findings based on sophisticated techniques should not be used as
a basis for classification, because these techniques are not
globally available.
10
Thus the current classification is still largely
based on basic histomorphology and requires proficiency in
routine diagnostic microscopy. Nevertheless, immunohisto-
chemical findings are still described, and where appropriate,
molecular changes are included because they enable more ac-
curate diagnosis of some SGT. Some of these will be discussed
below and are shown in Table 2, but it should be noted that, at
the present time, use of these adjunctive techniques is rarely
essential for diagnosis or management, although when present
they may define a particular entity. For example, two carcinomas
can be defined by specific gene translocations (secretory carci-
noma and clear cell carcinoma), while a number of other tu-
mours have molecular abnormalities that can assist diagnosis but
may not be consistently found (MEC, adenoid cystic carcinoma,
cribriform adenocarcinoma of minor salivary glands, PA and
sclerosing polycystic “adenoma”). As our understanding of these
molecular changes increases, we anticipate that genomic alter-
ations will become more important as diagnostic biomarkers and
that future classifications will become more reliant on molecular
changes, especially as many of these provide specific targets for
new therapies.
New entities
Secretory carcinoma
It has long been recognized that, occasionally, a tumour that
otherwise resembles acinic cell carcinoma (AcCC) does not show
the typical PAS-positive intracellular granules that defines acinic
differentiation. These were often referred to as “granule poor”
AcCC or relegated to the adenocarcinoma NOS category. In 2010
Skalova et al.
14
recognized that these neoplasms were similar to
secretory carcinoma of the breast and also shared the specific
ETV6-NTRK3 gene fusion. They called this tumour mammary
analogue secretory carcinoma (MASC) and it quickly became
established as a new entity with more than 250 cases now re-
ported. It is included in the WHO classification, under a new
simpler name, as secretory carcinoma (SC).
8
SC is found most
often in the parotid gland (70% of cases) with most of the
remainder arising in the buccal mucosa, lips and palate. Few
cases have been reported in the submandibular or sublingual
glands. Males appear to be slightly more often affected than fe-
males and there is a wide age range, with a number of cases
reported in children. Nodal metastases have been reported in up
to 25% of cases, but overall this is an indolent tumour with
survival exceeding 95%.
Key changes in the 2017 WHO classification of salivary
gland tumours
8
Key changes Explanatory notes
New entities
Secretory carcinoma First described in 2010.
14
Formerly
known as mammary analogue
secretory carcinoma (MASC)
Sclerosing
polycystic adenosis
First described in 1996.
15
There is
controversy over its status as a
neoplasm
New names
Polymorphous
adenocarcinoma
Formerly polymorphous low-grade
adenocarcinoma
Intraductal carcinoma Formerly low grade cribriform
cystadenocarcinoma, low grade
salivary duct carcinoma, salivary duct
carcinoma in situ
Poorly differentiated
carcinoma
Single category includes
undifferentiated carcinoma, large and
small cell neuroendocrine carcinoma
Clarifications, changes
Adenocarcinoma NOS Definition broadened to include rare
entities, including:
cystadenocarcinoma, mucinous (cyst)
adenocarcinoma, papillary
cystadenocarcinoma
Cystadenocarcinoma Cystadenocarcinoma is removed as a
separate entity (see above)
Mucinous adenocarcinoma Mucinous adenocarcinoma is
removed as a separate entity (see
above)
Metastasising pleomorphic
adenoma
Moved from malignant category to a
variant of benign pleomorphic
adenoma
Carcinoma ex-pleomorphic
adenoma
Clarifications on diagnostic
terminology: should explicitly state
the histological type of malignant
component.
Definition of minimally invasive
changed from 1.5 mm to “<4e6mm”
Sialadenoma papilliferum Given its own category. No longer a
“ductal papilloma”
Ductal papilloma A single name for two variants:
inverted ductal papilloma and
intraductal papilloma
Lymphadenoma A single category replacing sebaceous
and non-sebaceous lymphadenomas.
Sebaceous-type is regarded as a
simple variant
Non-neoplastic epithelial
lesions
New category, includes sclerosing
polycystic adenosis, nodular
oncocytic hyperplasia,
lymphoepithelial sialadenitis,
intercalated duct hyperplasia
Table 1
MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY
DIAGNOSTIC HISTOPATHOLOGY 26:4 148
Ó2020 The Authors. Published by Elsevier Ltd. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).

Antibodies that are useful in the diagnosis of salivary gland tumours
Antibody Target Diagnostic utility
Cytokeratins
CK7 Type II keratin. Mainly non-keratinising simple
epithelia
Virtually all SGT are positive for CK7. Useful to
confirm a salivary origin for unusual tumours
and metastases. If a tumour is CK7 negative,
first exclude an alternative diagnosis to SGT
CK20 Type I keratin. Mainly GI epithelium Virtually all SGT are negative for CK20. Useful
to exclude salivary origin for unusual tumours
and metastases. CK7/CK20 phenotypes define
many tumour types.
CK14 Myoepithelial cells Not entirely specific but marks myoepithelial
cells in most tumours. Useful for abluminal
cells in EMC.
AE1/AE3 Duct cells Stains most SGT. Useful to identify duct
(luminal cells) especially in EMC.
Myoepithelial markers
SMA Smooth muscle actin Reliable marker of mature myoepithelial cells.
Note that myoepithelial cells in PA (including
plasmacytoid cells) are largely negative. All
myoepithelial markers are useful in EMC and
for demonstrating peripheral cells around
tumour islands in intraductal (“in situ”)
carcinomas.
Calponin Basic smooth muscle protein Reliable myoepithelial cell marker. Stains
plasmacytoid cells in PA, so useful to use SMA
and calponin together.
p63 Transcription factor Reliable myoepithelial and basal cell marker.
Useful for EMC and stains peripheral cells in
AdCC, BUT not specific. Positive in other
tumours, in particular PAC (and CAMSG) shows
strong diffuse nuclear staining (and are p40-
negative). AcCC and SC are negative. p63 is
also a good marker for tumours of squamous
origin.
p40 An isoform of p63 Has very similar staining pattern as p63, BUT
PAC and CAMSG are negative. p63-positive/
p40-negative phenotype is useful for
diagnosis of PAC. Note that 26% of matrix-rich
PA may also be p40-negative.
SOX-10 Transcription factor Positive in most cells derived from neural
crest, but useful in PA and has a similar
distribution to DOG-1 in AcCC.
S100 Family of S100 proteins Traditionally a myoepithelial marker but lacks
specificity and little utility for myoepithelial
cells. Useful for diagnosis of SC and PAC where
it is strong and diffusely positive in 100% of
tumour cells. AcCC and AdCC are negative or
weak and patchy.
Cell cycle markers
Ki67/MIB-1 Cell cycle marker (G1/G2/S/M) Useful as indicator of malignancy and
aggression. High expression associated with
high grade lesions, BUT malignant SGT have
(continued on next page)
MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY
DIAGNOSTIC HISTOPATHOLOGY 26:4 149
Ó2020 The Authors. Published by Elsevier Ltd. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).

Histologically, SC shows features similar to AcCC with a
lobular growth pattern and microcystic, solid, follicular and
papillary cystic features. However, SC lacks the sheets of baso-
philic granular acinic cells that typify AcCC and the papillary
cystic pattern may be more common in SC. In our experience,
PAS (with diastase) staining is the single most useful diagnostic
aid.
9
In AcCC the acinic cells contain many PAS-positive gran-
ules, but the pale eosinophil cells in SC are negative. However, in
SC PAS does show a very characteristic globular staining within
the cystic and intercellular spaces. It was long felt that demon-
stration of the ETV6-NTRK3 gene rearrangement (by FISH) was
essential for diagnosis, but studies have now shown that there is
a characteristic immunohistochemical phenotype
16
that is almost
diagnostic and easily distinguishes SC from AcCC. SC shows
strong, diffuse positivity for S100 and mammaglobin, but is
negative for DOG-1. Conversely AcCC show consistent luminal
positivity for DOG-1 and SOX-10 but are negative or only patchily
positive for S100 and mammaglobin. More recently, a new
antibody has become available to tropomyosin receptor kinase
(pan-TRK) and this has been shown to be highly specific for the
diagnosis of SC.
17
In the field of precision medicine, TRK in-
hibitors (e.g. larotrectinib, entrectinib) have now been approved
for the clinical treatment of tumours with NTRK fusions regard-
less of their histology or site ea new tumour-agnostic approach
to therapy.
18
This will include SC and the results of ongoing
clinical trials may prove this to be an effective therapy.
Sclerosing polycystic adenosis
Although only about 60 cases of this controversial lesion have
been reported, sclerosing polycystic adenosis has been included
as a new entity. It was first described as an unusual inflammatory
or reactive disorder
15
that resembles fibrocystic disease of the
breast. It is almost exclusively found in the parotid gland, with
only occasional cases reported in the submandibular gland or
minor glands. The lesions are characterized by lobular areas of
densely collagenous fibrous tissue with multiple, cystically
dilated ducts, often with a cribriform or papillary cystic pattern.
Apocrine secretion, mucous cells, sebaceous cells and squamous
metaplasia may be seen as well as a chronic inflammatory cell
infiltrate. There is significant controversy over the nature of this
Table 2 (continued )
Antibody Target Diagnostic utility
notoriously low expression ee.g. very low in
cribriform AdCC and MEC.
MCM2 Cell cycle marker (G1/G2/S) Shown to always be >10% in AdCC but <10%
in PA and PAC. Useful in small biopsies where
there is a suspicion of AdCC.
Other markers
DOG-1 Luminal aspect of acini and small ducts Most useful for differentiation of AcCC from
SC. AcCC is positive, SC is negative.
Occasionally positive in ducts in a variety of
tumours including PA and AdCC. Occasionally
stains myoepithelial cells.
CD117 c-KIT (a tyrosine kinase) Not absolutely specific, but positivity suggests
AdCC (80%þof cases are positive)
PLAG1 PLAG1 protein Useful for diagnosis of PA, with positive
nuclear staining in about 95%. Rarely seen in
PAC and negative in AdCC.
GFAP Glial fibrillary acidic protein Useful marker for PA. It is almost always
positive, especially in myxoid areas. Rarely
seen in any other SGT.
Pan-Trk Tropomyosin receptor kinase New antibody that targets tumours with NTRK
fusion proteins. Useful for diagnosis of SC.
Mammaglobin Member of the uteroglobin family of
glycoproteins
Most useful for differentiation of AcCC from
SC; AcCC is negative, SC is strongly positive.
Myb Myb protein Positive in AdCC with the MYB-NFIB fusion.
Positive in about 65% of cases.
Androgen receptor Transcription factor Nuclear expression in 70% of salivary duct
carcinomas.
HER2 Epidermal growth factor receptor Positive in 25e30% of salivary duct
carcinomas, but also in high-grade intraductal
carcinoma.
AcCC, acinic cell carcinoma; AdCC, adenoid cystic carcinoma; CAMSG, cribriform adenocarcinoma of minor salivary gland; EMC, epithelial-myoepithelial
carcinoma; MEC, mucoepidermoid carcinoma; PA, pleomorphic adenoma; PAC, polymorphous adenocarcinoma; SC, secretory carcinoma.
Table 2
MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY
DIAGNOSTIC HISTOPATHOLOGY 26:4 150
Ó2020 The Authors. Published by Elsevier Ltd. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).

lesion, since some authorities regard the changes as neoplastic.
There is good evidence for this since lesions have been shown to
be monoclonal in nature and more recently it has been shown
that sclerosing polycystic adenosis shows genetic alterations in
the PI3K pathway and PTEN mutations.
19
This suggests that
these lesions are neoplasms. Intriguingly, although the WHO
classify it as a non-neoplastic epithelial lesion they give “scle-
rosing polycystic adenoma” as a synonym.
8
New names
Polymorphous adenocarcinoma
Polymorphous low grade adenocarcinoma was first named in
1984 as a low grade and indolent tumour, often found on the
palate. The lesion is widely infiltrative and often exhibits a
cribriform pattern similar to adenoid cystic carcinoma (AdCC),
with which it is often confused ehence the term “low grade”
was included in the name to clearly distinguish its behaviour
from that of AdCC. Previously we have noted that the behaviour
of this lesion can be unpredictable and some do not behave in a
low grade manner and we suggested the term “low grade” should
be removed from the name.
4
Although overall survival is better
than 95%, individual lesions can be unpredictable and lesions
may recur and metastasise. Recurrence rates of 5e33% have
been reported and about 10% overall show lymph node metas-
tases.
20
In effect the behaviour of the polymorphous “low grade”
adenocarcinoma was similar to MEC, yet even in 2005 the WHO
kept “low grade” in the name ethe only tumour to have its
grade defined in the name. In 2017 “low grade” has been drop-
ped and the new term for this tumour is polymorphous adeno-
carcinoma (PAC). Removing the term “low grade” will help
reduce inappropriate conservative management and ensure that
the lesion is managed in the same way as other malignant SGT,
based on clinical stage and a careful consideration of the histo-
logical features. Over 90% of PAC are found in the minor salivary
glands and it is the second most common intra-oral salivary
malignancy (after MEC), comprising about 40% of the total. It
most often occurs on the palate and females are affected almost
twice as often as males.
20
Histologically PAC shows a range of diverse morphological
features and diagnosis is based on recognition of these poly-
morphous features, which may only be apparent in a good-sized
biopsy or excision specimen. The features include a lobular
pattern, widespread infiltration, single cell filing and a charac-
teristic perineural infiltration with a whorling or targetoid pattern
(see below). A cribriform pattern is a common feature, which,
along with nerve involvement, is the main reason for misdiag-
nosis as AdCC (Figure 1). Many lesions also show a papillary
cystic morphology and it has been reported that these may be
more aggressive with a higher incidence of lymph node metas-
tases.
20
In 1999 a typically cribriform or papillary cystic variant
of PAC was reported in the tongue and was given the name
cribriform adenocarcinoma of the tongue ("CAT").
21
Subse-
quently lesions were reported at other intra-oral sites and the
tumour is now called cribriform adenocarcinoma of minor sali-
vary glands (CAMSG). This lesion was considered to be more
aggressive than PAC and many regard it as a new entity.
20,21
Its
distinction from PAC is supported by the finding that over 80% of
cases harbour rearranged PRKD1-3 genes compared to only 10%
of cases of PAC.
22
Conversely, more than 70% of PAC show a
specific PRKD (E710D) mutation which is only rarely seen in
CAMSG.
20,22
Controversially, the WHO specialist panel did not
include CAMSG as a new entity but rather considered it to be a
variant within the morphological spectrum of PAC (this is well
reviewed and critiqued by Vander Poorten et al.
20
). With some
justification this is based on the fact that they share similar
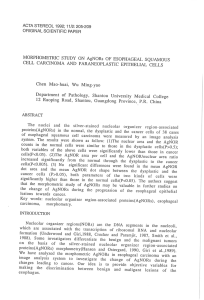
Figure 1 Four different tumours show a similar cribriform morphology, suggesting that simple “pattern-matching”is not appropriate in the
diagnosis of SGT. a) Polymorphous adenocarcinoma, b) canalicular adenoma, c) pleomorphic adenoma, d) adenoid cystic carcinoma.
MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY
DIAGNOSTIC HISTOPATHOLOGY 26:4 151
Ó2020 The Authors. Published by Elsevier Ltd. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).
 6
7
8
9
10
11
12
6
7
8
9
10
11
12
1
/
12
100%