High-Intensity Aerobic Exercise & Brain MRI in Multiple Sclerosis
Telechargé par
françois g

ARTICLE CLASS OF EVIDENCE
Efficacy of High-Intensity Aerobic Exercise on
Brain MRI Measures in Multiple Sclerosis
Martin Langeskov-Christensen, PhD, Lars Grøndahl Hvid, PhD, Mikkel Karl Emil Nygaard, MSc,
Steffen Ringgaard, PhD, Henrik Boye Jensen, MD, PhD, Helle Hvilsted Nielsen, MD, PhD,
Thor Petersen, MD, DMSc, Egon Stenager, MD, Simon Fristed Eskildsen, PhD, and Ulrik Dalgas, PhD
Neurology®2021;96:e203-e213. doi:10.1212/WNL.0000000000011241
Correspondence
Dr. Langeskov-Christensen
Abstract
Objective
To determine whether 24 weeks of high-intensity progressive aerobic exercise (PAE) affects
brain MRI measures in people with multiple sclerosis (MS).
Methods
We conducted a randomized, controlled, phase 2 trial (with a crossover follow-up) including an
exercise group (supervised PAE followed by self-guided physical activity) and a waitlist group
(habitual lifestyle followed by supervised PAE). Mildly to severely impaired patients with MS
aged 18–65 years were randomized (1:1). The primary outcome was percentage brain volume
change (PBVC) after 24 weeks, analyzed using the intention-to-treat principle.
Results
Eighty-six participants were recruited. PBVC did not change over the intervention period
(mean between-group change +0.12%, 95% confidence interval [CI] −0.27 to 0.51, p= 0.55). In
contrast, cardiorespiratory fitness (+3.5 mL O
2
/min/kg, 2.0 to 5.1, p< 0.01) and annualized
relapse rate (0.00, 0.00–0.07 vs +0.45, 0.28 to 0.61, p< 0.01) improved in the exercise group.
Conclusion
These findings do not support a neuroprotective effect of PAE in terms of total brain atrophy in
people with MS and it did not lead to a statistically significant difference in gray matter
parenchymal fraction. PAE led to improvements in cardiorespiratory fitness and a lower relapse
rate. While these exploratory findings cautiously support PAE as a potential adjunct disease-
modifying treatment in MS, further investigations are warranted.
Clinicaltrials.gov identifier
NCT02661555.
Classification of evidence
This study provides Level I evidence that 24 weeks of high-intensity PAE did not elicit disease-
modifying effects in PBVC in people with MS. Exploratory analyses showed that PAE may
reduce relapse rate.
MORE ONLINE
Class of Evidence
Criteria for rating
therapeutic and diagnostic
studies
NPub.org/coe
From the Section for Sport Science, Department of Public Health (M.L.-C., L.G.H., U.D.), and Center of Functionally Integrative Neuroscience, Department of Clinical Medicine
(M.K.E.N., S.F.E.), Aarhus University; MR Research Centre (S.R.) and Multiple Sclerosis Clinic, Department of Neurology (T.P.), Aarhus University Hospital; Brain and Nerve Diseases,
Department of Neurology (H.B.J.), Lillebaelt Hospital, Kolding; Department of Regional Health Research (H.B.J.), Department of Neurobiology Research, Institute of Molecular
Medicine (H.H.N.), BRIDGE–Brain Research–Inter-Disciplinary Guided Excellence, Department of Clinical Research (H.H.N.), and Department of Regional Health Research (E.S.),
University of Southern Denmark, Odense; Department of Neurology (H.H.N.), Odense University Hospital; and MS-Clinic of Southern Jutland (Sønderborg, Kolding, Esbjerg), De-
partment of Neurology (E.S.), Hospital of Southern Denmark, Sønderborg.
Go to Neurology.org/N for full disclosures. Funding information and disclosures deemed relevant by the authors, if any, are provided at the end of the article.
Copyright © 2020 American Academy of Neurology e203
Copyright © 2020 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Multiple sclerosis (MS) is a chronic neurodegenerative dis-
order of the CNS, causing motor, sensory, and cognitive
impairments.
1
Such disability progression is in part driven by
brain atrophy and focal lesions, which are quantifiable in vivo
by MRI.
2,3
Another measure of disease activity involves the
blood biomarker serum neurofilament light chain (sNfL),
4
a
promising marker reflecting neuroaxonal damage. Disease-
modifying treatments (DMTs) have been shown effective, but
MS remains an incurable and detrimental disease. It is thus
vital to identify adjuvant rehabilitative interventions with
disease-modifying effects.
Exercise is one potential intervention well-known to positively
affect MS symptoms.
5
Encouraging data from animal studies
along with human pilot/explorative studies suggest exercise to
be potentially disease-modifying or neuroprotective.
5–8
Indeed,
exercise has been demonstrated to positively alter brain MRI
measures (including brain volume)
5,6,9–13
and reduce relapse
rates.
5
Progressive aerobic exercise (PAE) has been proposed
to be particularly effective
9–11,13
and more so when performed
long-term.
14
Nonetheless, no long-term PAE study with MRI
disease progression measures as the primary outcome exists
in MS.
The primary purpose of the present study was therefore to
investigate whether 24 weeks of supervised high-intensity
PAE has neuroprotective effects on MRI measures in people
with MS (pwMS). A secondary purpose was to evaluate the
effects of PAE on sNfL, relapse rate, and functional and
patient-reported outcomes. We hypothesized that 24 weeks of
PAE would elicit disease-modifying effects, specifically in
percentage brain volume change (PBVC).
Methods
Standard Protocol Approvals, Registrations,
and Patient Consents
Ethics approval was obtained from the ethics committee of
the central Denmark region (record 1-10-72-291-15). The
study was registered in the database of the US National Li-
brary of Medicine (clinicaltrials.gov; NCT02661555) and
conducted in accordance with the Declaration of Helsinki. All
participants gave written informed consent before entry. The
Danish Data Protection Agency oversaw the study.
Study Design and Participants
A 24-week randomized, controlled, phase 2 trial (with a
crossover follow-up) was undertaken at the Section for Sport
Science, Aarhus University, Denmark, and at the Department
of Sports Science and Clinical Biomechanics, University of
Southern Denmark, Odense. The first part of the study
(i.e., 0–24 weeks) was a priori defined as the randomized
controlled trial (RCT) part; the remainder was follow-up.
The study design was chosen to ensure adherence (i.e., all
participants would receive the intervention), allow replication
and potential verification in the follow-up part, and to collect
follow-up data from the RCT intervention group. We have
previously published a study using baseline data examining
associations between cardiorespiratory fitness and cognitive
performance from these participants.
15
Participants were recruited from 4 Danish MS clinics located at
Aarhus University Hospital, Viborg Regional Hospital, Odense
University Hospital, and Kolding Hospital, Denmark, re-
spectively. For further details on inclusion and exclusion cri-
teria, see Langeskov-Christensen et al.
15
At inclusion, a
neurologist examined each participant to determine the Ex-
panded Disability Status Scale (EDSS) score, unless a recent
score (<6 months) followed by a disease-stable period until
trial start existed.
Randomization and Masking
Following inclusion and baseline testing, 2 researchers (M.L.-
C. or L.G.H.) randomly assigned participants (1:1) to an ex-
ercise or waitlist group using block randomization, stratified by
sex. Treatment assignment was balanced within each center.
Allocation was concealed by the sealed opaque envelope
principle. Participants were approved for participation and
enrolled via joint efforts of hospital neurologists and the prin-
cipal investigator. Patient and exercise supervisor masking were
not possible given the obvious differences between treatments.
MRI staffand laboratory technicians were masked to treatment
allocation when analyzing the primary outcome and blood
samples, respectively, and they had no interaction with patients
at any time during the study. Likewise, neurologists were
masked when assessing the number of confirmed relapses.
Procedures
The exercise group underwent 24 weeks of supervised long-
term PAE, whereas the waitlist group continued their habitual
Glossary
6MWT = 6-Minute Walk Test; ARR = absolute risk reduction; BPF = brain parenchymal fraction; DKI =diffusion kurtosis
imaging; DMT = disease-modifying treatment; EDSS = Expanded Disability Status Scale; FA = fractional anisotropy; FLAIR =
fluid-attenuated inversion recovery; GM = gray matter; GMPF = gray matter parenchymal fraction; HR
max
= maximum heart
rate; KFA = kurtosis fractional anisotropy; MD = mean diffusivity; MKT = mean kurtosis tensor; MS = multiple sclerosis;
MSIS = MS Impact Scale; NNT = number needed to treat; PAE = progressive aerobic exercise; PBVC = percentage brain
volume change; PRT = progressive resistance training; pwMS = people with multiple sclerosis; RCT = randomized controlled
trial; SIENA = structural imaging evaluation of normalized atrophy; sNfL = serum neurofilament light chain; WMPF = white
matter parenchymal fraction.
e204 Neurology | Volume 96, Number 2 | January 12, 2021 Neurology.org/N
Copyright © 2020 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

lifestyle (including ongoing physiotherapy treatment). After
cross-over, the exercise group was encouraged to continue
self-guided exercise, but without supervision or admittance to
the trial training facilities.
PAE sessions were conducted twice weekly between 1:00 and 6:
00 PM during the 24 weeks, comprising one continuous and one
interval exercise session. To ensureadherenceandaccurateex-
ercise progression, all sessions were supervised by exercise
physiologists. In brief, exercise volume increased from 30 to 60
minutes per session during the intervention period, while in-
tensity increased from 65% to 95% of the individual patient’s
maximum heart rate (HR
max
). Data available from Dryad (ap-
pendix, doi.org/10.5061/dryad.3ffbg79fs) provide details about
exercise modality options, volume and intensity progression of
the exercise sessions, and exercise intensity adherence.
At baseline (T0), after 24 weeks (T24), and after 48 weeks
(T48), the following parameters were assessed: MRI scans,
serum samples, cardiorespiratory fitness, walking capacity, and
a questionnaire to determine self-reported MS impact. Test
sessions, including MRI scans, were separated by a minimum of
48 hours and a maximum of 10 days from the last exercise bout.
All MRI measurements were performed on the same 3T MRI
scanner (Skyra; Siemens Medical Systems, Erlangen, Ger-
many). Structural T1-weighted MP2RAGE images, fluid-
attenuated inversion recovery (FLAIR) images, and diffusion
kurtosis imaging (DKI) were acquired. MP2RAGE and
FLAIR were 3D sequences. Data available from Dryad (ap-
pendix, doi.org/10.5061/dryad.3ffbg79fs) describe all details
about the MRI sequences and image processing.
Following 10–15 minutes of supine rest, serum samples were
obtained by a certified laboratory technician and stored at −80°C
according to standardized procedures.
16
Samples were collected
in the morning between 9:00 and 11:00 AM to minimize the
influence of circadian rhythms. An ultrasensitive single-molecule
array (Simoa) sNfL assay was used to explore longitudinal sNfL
development as previously described.
17
Participants performed an incremental exercise test until ex-
haustion on a bicycle ergometer to determine directly mea-
sured VO
2
max (Oxigraf O2CPX, Oxigraf Inc., Sunnyvale,
CA) and maximal cycling power output (W
max
). For further
details, see Langeskov-Christensen et al.
15
To objectively assess walking capacity, the 6-Minute Walk Test
(6MWT) was used. Participants were permitted habitual assistive
devices during testing and were instructed to complete the
6MWT “at their fastest speed and to cover as much distance as
possible”on a 30-meter hallway pivoting at each end of the hall.
The total distance walked after 6 minutes was registered.
The MS Impact Scale (MSIS)–29 physical and psychological
subscales were specifically selected to assess MS impact, thus
providing a subjective measure of disease impact/progression.
The number of confirmed relapses was obtained from the
patients’medical records.
Outcomes
The primary outcome was PBVC after 24 weeks, estimated by
structural imaging evaluation of normalized atrophy (SIENA).
18
Secondary MRI outcomes were normalized gray and white
matter volume (SIENAX),
18
brain parenchymal fraction (BPF),
gray matter parenchymal fraction (GMPF), white matter pa-
renchymal fraction (WMPF), cortical thickness, black hole le-
sion load (areas of focal axonal damage and irreversible tissue
destruction), volumes of hippocampus, thalamus, corpus cal-
losum, basal ganglia (defined as the caudate, putamen, and
globus pallidus), and upper spinal cord volume, T2 lesion load,
and DKI metrics (fractional anisotropy [FA], kurtosis fractional
anisotropy [KFA], mean diffusivity [MD], mean kurtosis tensor
[MKT]) of the cortex, hippocampus, thalamus, basal ganglia,
and corpus callosum. A secondary biomarker outcome was sNfL
concentration. The secondary clinical outcomes were cardio-
respiratory fitness (VO
2
max), W
max
,relapserate,6MWT,and
MSIS-29. Exercise adherence (% completed sessions) and ex-
ercise intensity were assessed. Adverse events were registered by
PAE supervisors.
Statistical Analysis
The sample size calculation (a 2-sample comparison of PBVC
means with 80% power to detect a treatment effect at a 5%
significance level while allowing for a 10% combined rate of
loss to follow-up and nonadherence) was applied (control
mean PBVC = −0.27859 ± 0.5253; experimental mean PBVC
=−0.0129 ± 0.2698),
12
revealing that a total of 86 pwMS were
needed.
Descriptive baseline variables modeled as continuous (i.e., age,
height, weight, body mass index, EDSS, time since diagnosis,
cardiorespiratory fitness, cycling power output) were assumed
to follow a normal distribution. All analyses were performed
using an intention-to-treat linear mixed effects model including
all randomized participants. Patients who dropped out con-
tributed with information in their respective groups until they
dropped out (i.e., imputation was not applied). The primary
outcome was analyzed with group as a fixed effect and patient ID
as a random effect, since PBVC reflects changes between time
points (i.e., change from T0 to T24 and from T24 to T48).
Secondary longitudinal data were analyzed using a mixed-effects
analysisforrepeatedmeasureswithtimeandgroupasfixed
effects and patient ID as a random effect. To account for mul-
tiple comparisons, we also present Bonferroni-corrected
between-group findings. Likelihood ratio tests were used to
test for equal/unequal SDs and correlations in the 2 groups for
each secondary outcome. Model validation was performed by
inspecting the standardized residuals (i.e., QQ-plots, plots of the
standardized residuals against the fitted values). Data were log-
transformed when appropriate (sNfL, black hole lesion load)
but presented as raw point values. Log-transformed between-
and within-group changes were back-transformed by the ex-
ponential function to median ratios. If a significant time × group
Neurology.org/N Neurology | Volume 96, Number 2 | January 12, 2021 e205
Copyright © 2020 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

interaction was found, linear combinations of estimates were
used to compute point estimates of group changes of interest
(e.g., comparison of exercise and waitlist group changes from T0
to T24). Within-group changes in the RCT part were only
tested (using unadjusted post hoc linear pairwise comparisons)
if a significant time by group interaction was found but linear
combinations of estimates showednobetween-groupeffect.
RCT intervention group follow-up data were analyzed using
unadjusted post hoc linear pairwise comparisons to test within-
group changes.
The unadjusted annualized relapse rate was calculated by
dividing the total number of relapses by the number of
relapsing-remitting patients in the group, giving a mean re-
lapse rate, and then extrapolating to an annualized rate by
correcting for the time period during which the relapses were
observed (i.e., 24 weeks). Since a relapse did not occur in the
exercise group, we applied “the rule of 3”in the RCT part of
the study to calculate an approximate CI for this outcome
(with zero events out of n, a 95% upper confidence limit for
the true proportion is determined from 3/n).
19
Given the
relapse rate of zero, annualized relapse rates were compared
with a 2-sample test of proportions.
Absolute risk reduction (ARR) and number needed to treat
(NNT) for the main outcome were defined according to a
cutoffvalue of −0.4% per year that discriminates between
“physiologic”or “pathologic”PBVC in pwMS.
20
As numerous cortical segments exist, cortical DKI and thick-
ness were explored using surface-based statistical analysis. The
cortical maps were analyzed with a general linear mixed effects
model with age, sex, and group as fixed effects using the SurfStat
toolbox
21
in MATLAB 2016b (The MathWorks, Inc., Natick,
MA). The statistical maps were family-wise error corrected
using random field theory with a cluster-defining threshold of
α= 0.001 to account for multiple comparisons. The produced
maps were visualized by Persistence of Vision Raytracer
(povray.org/).
Graphs were made using GraphPad Prism version 8.0.1
(GraphPad Software). Statistical calculations were performed
in Stata version 15.1 (StataCorp LP). Statistical significance
was set at p≤0.05.
Classification of Evidence
This randomized, controlled, phase 2 trial assessed the effi-
cacy of supervised long-term high-intensity PAE for reduction
of brain atrophy in mildly to moderately impaired pwMS. This
study provides Class I evidence that 24 weeks of high-
intensity PAE did not elicit disease-modifying effects in
PBVC. Exploratory analyses showed that high-intensity PAE
may reduce relapse rate in pwMS.
Data Availability
The data that underlie the results reported in this article will be
made available beginning 6 months and ending 5 years after
article publication. Access will be given, on reasonable request,
to investigators whose proposed use of the data has been ap-
proved by a review committee identified by the authors of this
study. Once access is granted, data will be available through
The Danish National Archives at sa.dk/en/ (please contact the
corresponding author at mach@ph.au.dk).
Results
Baseline (T0)
Participants were recruited between 28 April 2016 and 10
October 2017. Among the 148 patients invited to participate,
86 were enrolled and assessed for the primary and secondary
outcomes (figure 1). There were 13 dropouts after 24 weeks
(15.1%) and 9 additional dropouts after 48 weeks, producing a
total dropout of 22 (25.6%; see figure 1). The patient pop-
ulation had a representative distribution of relapsing-remitting
(87.2%) and progressive (12.8%) patients. Most patients were
receiving DMTs for MS, with no differences in type or pro-
portion between groups. Baseline demographic and clinical
characteristics of the study population are shown in table 1.
Effects of PAE in the RCT (T0–T24)
The primary efficacy outcome was PBVC from T0 to T24
(table 2 and figure 2A). After 24 weeks, there was no difference
intheestimatedPBVCintheexercisegroupvsthewaitlist
group (between-group change +0.12%, 95% CI −0.27 to 0.51, p
=0.55).ARRandNNTforPBVCwere0.07(i.e.,7%)and14.3
(i.e., 15 patients), respectively. The secondary outcomes
showed a higher GMPF (+1.13 percentage point, 0.00; 2.26, p=
0.05; did not remain after Bonferroni correction), cardiorespi-
ratory fitness (+3.5 mL O
2
/min/kg, 2.0 to 5.1, p<0.01),and
maximal cycling power output (+24.0 watts, 16.5 to 32.5, p<
0.01) among PAE than among waitlist patients (tables 2 and 3
and figure 2D). Furthermore, the change in black hole lesion
load was more extensive in the exercise group than in the waitlist
group after 24 weeks (+12%, 3–21, p= 0.01; did not remain
after Bonferroni correction). No additional within- or between-
group volumetric MRI changes were observed following the 24-
week RCT intervention period. In addition, sNfL levels and
MSIS-29 developed similarly over the 24 weeks in the 2 groups
(table 3). The number of relapses was significantly lower in the
exercise group, experiencing zero relapses, than in the waitlist
group, which saw 7 relapses (p< 0.01). Also, the unadjusted
annualized relapse rates of zero (0.0–0.07) in the exercise group
and +0.45 (0.28–0.61) in the waitlist group were significantly
different (p< 0.01). A within-group time effect was observed,
showing improved walking capacity (6MWT) in the exercise
group after 24 weeks (+27.2 meters, 13.8–40.5, p< 0.01).
Exploratory cortical statistical maps of thickness and DKI
revealed no compelling between-group patterns suggesting
any superior effects of PAE over waitlist (data available from
Dryad, appendix, doi.org/10.5061/dryad.3ffbg79fs). Simi-
larly, regional mean DKI estimates (FA, KFA, MD, MKT)
from the hippocampus, thalamus, putamen, globus pallidus,
e206 Neurology | Volume 96, Number 2 | January 12, 2021 Neurology.org/N
Copyright © 2020 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

and corpus callosum showed no between-group changes.
While MD and MKT developed equally in the caudate in both
groups, FA (−0.01, −0.03; 0.00, p= 0.04; did not remain after
Bonferroni correction) and KFA (−0.02, −0.05; 0.00, p= 0.05;
did not remain after Bonferroni correction) significantly de-
creased in the exercise group.
The adherence analysis showed that the exercise group
completed 44.8 (2.6) sessions (93.3% [5.4]) and participated
in 22.4 (1.8) continuous exercise sessions (93.6% [7.6]) and
22.2 (1.6) interval exercise sessions (92.6% [6.9]). Twelve
participants were unable to complete the intervals at the
prescribed intensity of 90%–95% of HR
max
during the last 8
weeks of the intervention (mean intensity for the 12 partici-
pants: 87.8% of HR
max
). The PAE intervention was well tol-
erated, with no serious adverse events. Adverse events
comprised 3 cases of severe physical fatigue.
To further explore the change in GMPF in the exercise group
after the first 24 weeks, we conducted a post hoc analysis,
demonstrating a significant correlation between GMPF change
and cardiorespiratory fitness change from T0 to T24 in the
total population (r=0.23,p= 0.05). Lastly, in order to rule out
the MS phenotypic distribution in the trial groups, a post hoc
analysis was performed including MS type as a covariate in the
linear mixed effects model, showing no changes in regards to
the significant findings of the present trial.
Effects of Delayed PAE in the Waitlist
Group (T24–T48)
The study design allowed us to replicate and verify the in-
tervention group findings from the RCT part in the waitlist
group as well (i.e., undergoing PAE from T24–T48). The
pattern of changes was replicated and verified for all out-
comes, except for mean corpus callosum volume (+0.02 cm
3
,
0.00–0.03, p= 0.02; did not remain after Bonferroni correc-
tion) and thalamus MD (+0.04, 0.00–0.08, p= 0.05; did not
remain after Bonferroni correction), where the waitlist group
increased more. Also, there was a trend in sNfL (−13%, −25;
0, p= 0.06) towards a better intervention effect in the waitlist
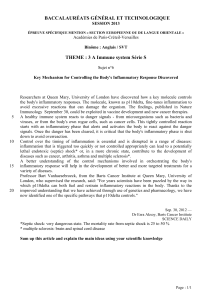
Figure 1 Trial Profile
“Worsening of symptoms”covers worsening of walking or vision. Dropouts due to physical problems, except for “physical fatigue,”were not related to the
exercise intervention. MS = multiple sclerosis.
Neurology.org/N Neurology | Volume 96, Number 2 | January 12, 2021 e207
Copyright © 2020 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
 6
7
8
9
10
11
6
7
8
9
10
11
1
/
11
100%