The Scientific World Journal - 2024 - Valentin - Ethnomedical Knowledge of Plants Used in Nonconventional Medicine for
Telechargé par
bashige.chiribagula

Research Article
Ethnomedical Knowledge of Plants Used in Nonconventional
Medicine for Wound Healing in Lubumbashi, Haut-Katanga
Province, DR Congo
Bashige Chiribagula Valentin ,
1
Okusa Ndjolo Philippe ,
1
Manya Mboni Henry ,
1
Bakari Amuri Salvius,
2
Masengu Kabeya Suzanne,
1
F´
elicien Mushagalusa Kasali ,
3
and Lumbu Simbi Jean Baptiste
4
1
Department of Pharmacology, Laboratory of erapeutic Chemistry and Analysis of Natural Substances,
Faculty of Pharmaceutical Sciences (UNILU), 27, Av. Kato, Commune Kampemba, Lubumbashi,
Democratic Republic of the Congo
2
Department of Pharmacology, Laboratory of Pharmacognosy, Faculty of Pharmaceutical Sciences,
University of Lubumbashi (UNILU), 27, Av. Kato, Commune Kampemba, Lubumbashi, Democratic Republic of the Congo
3
Department of Pharmacy, College of Health Sciences, Universit´e Ocielle de Bukavu (UOB), PO. Box: 570, Bukavu,
Commune of Kadutu, Av. Karhale, Democratic Republic of the Congo
4
Department of Chemistry, Faculty of Sciences, University of Lubumbashi (UNILU), 1 Maternity Av., Commune of Lubumbashi,
Lubumbashi, Democratic Republic of the Congo
Correspondence should be addressed to Bashige Chiribagula Valentin; [email protected]
Received 24 May 2024; Accepted 16 July 2024
Academic Editor: Neeraj S. akur
Copyright ©2024 Bashige Chiribagula Valentin et al. is is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Medicinal plants used for wound healing in Lubumbashi have yet to be discovered. Inventory or prole of their taxa has yet to be
established. e present study was carried out to survey the plants used in traditional medicine in Lubumbashi to treat wounds
and to dene their ethnomedical characteristics. e study was conducted between March 2021 and August 2022, using
semistructured interview surveys of households (n= 2730), herbalists (n= 48), and traditional practitioners: TPs (n= 128).e
2,906 interviewed (sex ratio M/F = 0.9; mean age: 56 ±3 years; and experience: 17 ±4 years) provided information on 166 taxa, 130
used against chronic wounds, among which Securidaca longepedunculata was the top cited. Most of these taxa are shrubs (33%),
belonging to 48 botanical families dominated by the Fabaceae (16%). ey are indicated in 70 other pathologies. From these 166
taxa, 198 healing recipes are obtained, 11 combining more than one plant. In all these recipes, the leaf (>36%) is the most used part,
and the poultice (>36%) is the most popular form of use. Twelve taxa are cited for the rst time as medicinal plants, of which
Agelanthus zizyphifolius has the highest consensus and Erigeron sumatrensis has the highest usual value. For the various plants
used to treat wounds, some of which are specic to the region, further studies should focus on validating this traditional use.
1. Introduction
A wound disrupts routine, typical standard anatomical
tissue structure, resulting in loss of epithelial continuity with
or without loss of underlying connective tissue and living
tissue’s anatomical and functional integrity [1, 2]. Dierent
types of wounds, including incised wounds, lacerated
wounds, abrasions, contusions, ulcers, and burns, can be
distinguished according to their origin, duration, and
healing process and grouped into acute and chronic wounds
[1, 3]. In response to this structural damage, the body ini-
tiates wound healing, a natural process of repair and re-
generation of tissue lesions that includes the phases of
hemostasis (coagulation), inammation, proliferation
Wiley
The Scientific World Journal
Volume 2024, Article ID 4049263, 33 pages
https://doi.org/10.1155/2024/4049263

(angiogenesis, granulation, and reepithelialization), and
tissue remodeling [4, 5].
Wounds that have not followed the normal healing
process and remain open for more than a month or whose
size has not contracted by more than 50% during this period
are considered chronic wounds [6–8]. Based on etiology, the
Wound Healing Society classies chronic wounds into four
categories: pressure ulcers, diabetic ulcers, venous ulcers,
and arterial insuciency ulcers [9]. Chronic wounds cause
severe emotional and physical trauma for not only the
patient but also their family [10, 11]. Chronic wounds can
also lead to disability after all available therapeutic in-
terventions have been exhausted and amputation deemed
necessary [10, 12]. e worldwide prevalence of chronic
wounds is estimated at 1.51 and 2.21 per 1000 inhabitants
[13], and 1 to 2% of the population in developed countries
has already been diagnosed with chronic wounds [14]. is
rate is three times higher in DRC, where access to primary
healthcare and hospital technical facilities suers enormous
shortcomings. Incidence is set to rise as populations age
worldwide [15], and the risk of developing a chronic wound
is 1.72 times higher in men than in women [16]. Chronic
wounds are, therefore, a signicant health problem with
various consequences, aecting patients’ physical, social,
and mental health as well as the costs of healthcare systems.
eir prolonged healing time, economic burden, reduced
quality of life, increased risk of infection, and impact on
patient mobility and functionality make them a signicant
concern for healthcare professionals [17]. In Lubumbashi,
there are many cases of chronic wounds, due to the high level
of mining activity and other physical activities, combined
with poor access to adequate care, which favors cases of
infected wounds [18].
e current therapeutic arsenal oered by conventional
medicine is varied, ranging from regenerative medicine and
stem cell therapies to biological dressings and scaolds,
negative pressure wound therapy (NPWT), electrical stim-
ulation, topical growth factors and cytokines, hyperbaric
oxygen therapy (HBOT), advanced dressings, and articial
intelligence [9, 17]. Despite the existence of these treatment
methods, chronic wounds are among the pathologies for
which the people of Lubumbashi most often turn to non-
conventional medicine as in many cases biomedical treat-
ment has resulted in therapeutic failure on the one hand, but
on the other, the population has more condence in al-
ternative medicine due to sociocultural habits [18, 19]. In
addition to the abovementioned reasons, it should be re-
membered that the DRC, particularly the city of Lubum-
bashi, suers from poor health coverage. e low rate of
access to primary health care could also justify the high
demand for nonconventional medicine [18]. is non-
conventional medicine remains dominated mainly by me-
dicinal plants and is poorly documented in
Lubumbashi [20].
e ethnomedical use of plants in wound treatment is
not only cheap and accessible but also a reliable natural
resource of medicinal substances. Studies on medicinal
plants have conrmed that herbal medicines have fewer side
eects than chemical agents and are more cost-eective
[21–23]. As medicinal plants constitute an essential re-
source of substances with benecial therapeutic eects, in
various African countries, plants with wound-healing po-
tential have been investigated from both the ethnobotanical
and ethnopharmacological points of view [24–27].
A link between ethnopharmacological activity and
bioactive groups has justied the traditional use of some
medicinal taxa for wound treatment [28–31], and several
phytomedicines have been developed, such as Cicaplast®
used for the treatment of acute wounds [32] and Cicatryl®
used for the treatment of supercial wounds [33].
In DRC, to our best knowledge, a single ethnobotanical
survey was carried out on wound-healing medicinal plants.
It reported 53 taxa used as healing plants in Congolese
pharmacopeias [34]. Examination of this study shows that
the taxa described tend to come from the western part of the
DRC, which is not representative of the whole country due
to the climatic variability that characterizes each region of
the country. is is particularly true of Haut-Katanga
Province, where the Miombo Forest is characterized by
other types of vegetation, and the population living there has
dierent cultural practices to those found in the west of the
country.
e present study aims to inventory the plants and
their healing recipes used in nonconventional medicine
in Lubumbashi and to draw up their ethnomedicinal
characteristics. Aware that the general population
practices this medicine, traditional healers and herbalists,
we have focused the study on three population categories
(households, herbalists, and traditional healers) to gather
as much information as possible about wound care in the
region.
2. Materials and Methods
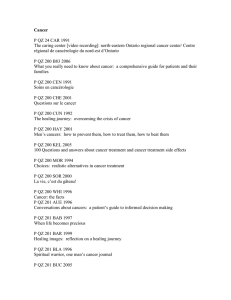
2.1. Experimental Framework. is study was conducted in
the seven communes of Lubumbashi City: Annexe, Kam-
pemba, Katuba, Kamalondo, Kenya, Lubumbashi, and
Rwashi, in the province of Haut-Katanga in the Democratic
Republic of Congo.
Lubumbashi is located between 11°26′–11°55′north
latitude and 27°15′–27°40′east longitude at an altitude of
1,230 meters. e climate is tropical, with an average annual
temperature of 22.4°C and an average annual rainfall of
512.7 mm
3
. It has two seasons, with a shorter rainy season
(November to April). e Miombo clear forest dominates
typical vegetation [35] (Figure 1).
2.2. Ethnomedical Data Collection. Ethnobotanical data
were collected from households, herbalists, and tradi-
tional practitioners (TPs) in Lubumbashi between March
2021 and August 2022. e sample size of household
respondents was determined using two-stage sampling:
a stratied sample and a cluster sample. For each com-
mune considered a stratum, the corresponding commune
oce provided the population size. e size of the rep-
resentative sample at this level was determined by the
following formula [36]:
2e Scientic World Journal
8086, 2024, 1, Downloaded from https://onlinelibrary.wiley.com/doi/10.1155/2024/4049263 by Bashige Chiribagula - EBMG ACCESS - CONGO, DEM REP , Wiley Online Library on [12/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License

n�t2
p∗p(1−p)∗N
t2
p∗p(1−p) +(N−1)∗y2,(1)
where nis the sample size, Nis the actual population size, p
is the expected proportion of respondents (we estimated pat
0.5), tpis the sampling condence interval (tp�1.96 given
that we set a 95% condence interval), and yis the margin of
sampling error: we put it at 0.05.
For this study, given that for a population of over 20,000
households, the sample size varies little for margins of error
greater than 5%, and we adjusted the minimum size with an
excess of over 1.5% (Table 1).
e sample determined by commune was divided by
avenue, considered clusters by counting every three
households. In each household, we included any adult
(≥18 years old) who had ever used plants to treat wounds,
provided they were too unfamiliar with the interviewers.
Due to a lack of reliable data on the size of the herbalist
population in Lubumbashi, we aimed to interview as many
herbalists as possible, accessible through markets and other
public spaces. is stage enabled us to meet 48 herbalists
who agreed to participate in the study.
Respondents in the traditional practitioner category
were determined from a list of 50 TPs drawn up during
a recent survey in the study region [35]. is stage resulted in
45 TPs, all of whom agreed to participate. From them,
snowball sampling was carried out to increase the sample
size, which enabled us to reach a further 85 TPs, 83 of whom
agreed to participate in the study and 4 of whom were on the
initial list. e TP survey was thus carried out on 128
respondents.
2.3. Data Processing and Analysis. During the surveys, the
plants were identied in the local languages. e specimens
were collected in the company of the informants, and
herbaria were compiled and deposited at the Kipopo Her-
barium for the attribution of scientic names. Subsequently,
these records were updated through comparison with the
following databases: the African Plant Database (https://
africanplantdatabase.ch/) Plants of the World Online
(https://powo.science.kew.org/) and the World Flora Online
(http://www.worldoraonline.org/).
Annexe
Kamalondo
Kampemba
Katuba
Kenya
Lubumbashi
Ruashi
Figure 1: Map of the city of Lubumbashi in Haut-Katanga, DRC.
Table 1: Household sample size.
Commune NncneDierence (%)
Annexe 749142 384.0 391 1.8
Kamalondo 27911 379.0 389 2.6
Kampemba 526 926 383.9 390 1.6
Katuba 469228 383.8 390 1.6
Kenya 480974 383.9 390 1.6
Lubumbashi 481563 383.9 390 1.6
Rwashi 410 034 383.8 390 1.6
Total 3 145 778 2 682 2 730 1.8
N: target population; nc: calculated representative sample; and ne: pop-
ulation surveyed in the eld.
e Scientic World Journal 3
8086, 2024, 1, Downloaded from https://onlinelibrary.wiley.com/doi/10.1155/2024/4049263 by Bashige Chiribagula - EBMG ACCESS - CONGO, DEM REP , Wiley Online Library on [12/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License

ree ethnomedicinal indexes were determined to assess
signicant species (data): the therapeutic consensus index
(TCI), the medicinal usage index (MUI), and the medicinal
capability index (MCI). e plant therapeutic consensus
index (TCI) was calculated using the formula:
TCI �Np
N,(2)
where Np is the number of people who mentioned the plant
and Nis the number of people surveyed during the study.
e medicinal use index (MUI) was calculated using the
formula:
MUI �NUi
Up,(3)
where NUi is the number of uses of plant iand up is the set
of uses of all plants inventoried during this study. e
medicinal capability index (MCI) was calculated by the
formula:
MCI �nt
Nt,(4)
where nt is the number of taxa cited in the management of
a given pathology and Nt is the total number of taxa in-
ventoried during the study.
In addition to the three ethnomedicinal indexes men-
tioned above, the relative citation frequency (RCF) was also
determined. It was calculated using the formula:
RCF �n
N×100,(5)
where nis the number of occurrences of the factor examined
and Nis the total number of the population concerned. is
parameter was used to quantify various factors analyzed in
this study, except for those for which ethnobotanical indexes
were applied.
In this study, the MUI highlights the level of medicinal use
of a plant among the population studied; TCI enables us to
identify the level of consensus among the population on the
healing use of a given species and, hence, its importance in
managing wounds in the region. As this is a targeted ethno-
botanical study, the medicinal consensus index corresponds to
citation frequency. MCI enables us to measure the potential of
a given community to manage a well-dened pathology.
3. Results
3.1. General Characteristics of Inventoried Plants. is study
identied one hundred and sixty-six plant species used as
healing plants in Lubumbashi, 130 of which are used to treat
chronic wounds. ese plants were collected from house-
holds, traditional practitioners, and herbalists. Depending
on the origin of the information obtained for each taxon
during the surveys, we can group the plants inventoried
during this study into 6 classes: u,w,v,x,z, and y(Figure 2).
(i) Class u, made up of 15 taxa from households
alone, where Securidaca longepedunculata,
Musa ×paradisiaca, Manihot esculenta, Jatropha
curcas, and Tetradenia riparia occupy the top ve
positions according to their TCI: therapeutic
consensus index (0.306–0.689)
(ii) Class w, comprising 68 taxa from traditional
practitioners alone, where Sterculia quinqueloba,
Ziziphus abyssinica, and Triumfetta rhomboidea
occupy the top 3 positions in terms of TCI
(0.027–0.043)
(iii) Class v, comprising 38 taxa from herbalists alone,
with Annona senegalensis,Dysphania ambrosioides,
Albizia antunesiana,Chenopodium opulifolium, and
Crossopteryx febrifuga in the top 5, with MCIs
(medicinal capability indexes) ranging from 0.014
to 0.017
(iv) Class x, comprising 24 taxa from both traditional
practitioners and herbalists, where Sterculia quin-
queloba,Ziziphus abyssinica,Triumfetta rhomboi-
dea,Uapaca sansibarica, and Terminalia mollis
occupy the top 5 positions (TCI: 0.013–0.024)
(v) Class z, comprising 9 taxa from both traditional
practitioners and households, where the top 5 po-
sitions are occupied by Acalypha cupricola,Acaly-
pha homblei,Acalypha ornata,Acalypha chirindica,
and Vachellia karroo, with a TCI varying between
0.046 and 0.081
(vi) Class y, comprising 13 taxa common to all 3 sources,
of which the top 5 according to their MCI values
(0.048–0.087) include Allium sativum,Bobgunnia
madagascariensis,Ficus sur,Euphorbia hirta, and
Cassia abbreviata (Table 2)
ese taxa belong to 48 families (Table 2), only 13 of
which contain at least 3 taxa among those inventoried during
this study. ese families are dominated by the Fabaceae (27
taxa), followed by the Phyllanthaceae and Euphorbiaceae
with 20 taxa each. e Asteraceae family ranks fourth with
15 taxa, followed by the Rubiaceae with 7 (Figure 3(a)). Each
of these inventoried plants is named in one of the languages
of the 26 Congolese ethnic groups, of which Bemba (31%),
Shi (14%), Luba-Kat (12%), Swahili, and Kikongo, with an
RCF of over 8% each, occupy the top ve places
(Figure 3(b)).
Nine plants are the most widely used in the study area,
with the medicinal usual index: MUI >0.090. ese are, in
order of precedence, Lantana camara (0.194), Gardenia
ternifolia (0.181), Tetradenia riparia (0.139), Xylopia
aethiopica (0.139), Euphorbia hirta (0.125), Garcinia huil-
lensis (0.111), Cucumis melo (0.111), Curcuma longa (0.097),
and Nauclea latifolia (0.097) (Table 2).
ese plant taxa comprise 7 morphological types,
dominated by the shrub type (33%), followed by the tree
type, which represents 27% of taxa (Figure 3), and also
include 15 geographical types, dominated by the in-
tertropical African type, which shall consist of 32% of taxa
(Figure 4).
Of the 166 taxa listed, Securidaca longepedunculata
(0.689), Musa ×paradisiaca (0.642), Manihot esculenta
(0.353), Jatropha curcas (0.314), and Tetradenia riparia
4e Scientic World Journal
8086, 2024, 1, Downloaded from https://onlinelibrary.wiley.com/doi/10.1155/2024/4049263 by Bashige Chiribagula - EBMG ACCESS - CONGO, DEM REP , Wiley Online Library on [12/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License

(0.306), with a therapeutic consensus index: TCI >0.3, are
the most consensual and most cited as healing plants for this
study. ey all come from class w, a class dedicated to plants
sourced solely from resource persons encountered in
households (Table 2).
e literature consulted in relation to the 166 taxa in-
ventoried during the surveys shows that one hundred and
eighteen taxa (71%) have never been studied from the point
of view of assessing their healing activity. Of these, 70 are
reported for the rst time as plants used in wound care,
including 12 taxa reported for the rst time as medicinal
plants, of which Agelanthus zizyphifolius (MCI �0.042) has
the highest consensus factor and Erigeron sumatrensis (5
uses) has the highest usual value. ese taxa are used in the
management of chronic wounds (Table 2).
3.2. Ethnomedical Prole of Inventoried Plants. e 166
plants identied in this study during the surveys are used in
198 healing recipes, of which 187 use a single plant (Table 2)
and 11 combine two plants (Table 3). In these essentially
topical recipes, the leaf is the organ most frequently used
(36.9% in monophytotherapy and 75% in biphytotherapy).
Root barks follow it in monophytotherapy and roots in
biphytotherapy. Cataplasm is the most frequently used form
of administration (36.4% for monophytotherapy and 50%
for biphytotherapy), followed by ointment (Figure 5).
In monophytotherapy, recipes based on Securidaca
longepedunculata (root bark), Musa ×paradisiaca (leaves),
Manihot esculenta (leaves), Jatropha curcas (leaves), and
Tetradenia riparia (leaves) are the most widely accepted,
with TCI >0.3 (Table 2). In the polyherbal recipe, the recipe
based on a mixture of Moringa oleifera (leaves) and Garcinia
guillen (root bark) with a TCI of 0.33 was the most widely
cited. e taxa, Ageratum conyzoides,Euphorbia hirta,
Garcinia huillensis, and Moringa oleifera, are each used in 2
dierent recipes for plants used in mixtures (Table 3).
e taxa inventoried in this study are involved in the
management of 70 other pathologies, of which fever,
malaria, DTIs (digestive tract infections), diabetes, and
STIs (sexually transmitted infectious diseases), with a RCF
≥40% of subjects consulted, are the most cited. However,
diabetes, DTI, malaria, STIs, diarrhea, fever, and dysen-
tery are the conditions with the highest potential for
medicinal treatment in the study region, MCI:
0.102–0.259 (Table S1).
3.3. Sociodemographic Prole of Interviewed Subjects. e
persons consulted in this study were either household
contacts (93.9%), herbalists (1.7%), or practitioners of tra-
ditional medicine (4.4%), primarily women (56.4%), most of
whom were between 50 and 60 years old (extremes: 18 and
71). e majority had a secondary education (39.0%). ese
persons were found in the 44 districts that make up the seven
communes of the city of Lubumbashi in similar proportions
(13.9–15.1%). ey were engaged in 6 occupation types, the
most representative of which was housework (52.6%). In
most cases, they have more than 11 years of experience using
medicinal plants (Table 4).
4. Discussion
Katangese ora is rich in plant taxa, the ethnomedical
knowledge of which needs to be better reported. rough
this study, we propose to report on ethnomedical
Class w
15 taxa
68 taxa
38 taxa
Households
n= 2730
Traditional
healers
n=59
Herbalists
n=25
9 taxa
24 taxa
0 taxon
13 taxa
Class y
Class z
Class x
Class t
Class v
Class u
Figure 2: Distribution of taxa by informant source.
e Scientic World Journal 5
8086, 2024, 1, Downloaded from https://onlinelibrary.wiley.com/doi/10.1155/2024/4049263 by Bashige Chiribagula - EBMG ACCESS - CONGO, DEM REP , Wiley Online Library on [12/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
1
/
33
100%