Original Research
A School- and Home-Based Intervention
to Improve Adolescents’ Physical Activity
and Healthy Eating: A Pilot Study
Lorraine B. Robbins, PhD, RN, FNP-BC, FAAN
1
, Jiying Ling, PhD, RN
1
,
Kimberly Clevenger, MS
2
, Vicki R. Voskuil, PhD, RN, CPNP
3
,
Elizabeth Wasilevich, PhD, MPH
1
, Jean M. Kerver, PhD, RD
4
,
Niko Kaciroti, PhD
5,6
, and Karin A. Pfeiffer, PhD
2
Abstract
This study evaluated feasibility, acceptability, and preliminary efficacy of a 12-week Guys/Girls Opt for Activities for Life (GOAL)
intervention on 10- to 13-year-old adolescents’ body mass index (BMI), percent body fat, physical activity (PA), diet quality, and
psychosocial perceptions related to PA and healthy eating. Parent–adolescent dyads from two schools were enrolled. Schools
were assigned to either GOAL (38 dyads) or control (43 dyads) condition. The intervention included an after-school club for
adolescents 2 days/week, parent–adolescent dyad meeting, and parent Facebook group. Intervention adolescents had greater
autonomous motivation for PA and self-efficacy for healthy eating than control adolescents (both p< .05). Although between-
group differences were not significant, close-to-moderate effect sizes resulted for accelerometer-measured moderate-to-
vigorous PA and diet quality measured via 24-hr dietary recall (d¼.46 and .44, respectively). A trivial effect size occurred
for percent body fat (d¼.10). No differences emerged for BMI. Efficacy testing with a larger sample may be warranted.
Keywords
diet, exercise, nutritional status, obesity, overweight, parent, social media, social support, school nursing
Health-promoting interventions are particularly needed for
underserved (minority and/or low income) adolescents in
urban areas who have a higher risk for becoming overweight
(OW) or obese (OB) due to greater barriers practicing a
healthy lifestyle compared to other adolescents (O’Haver,
Jacobson, Kelly, & Melnyk, 2014). Although schools are
an ideal setting for reaching at-risk adolescents (Nordin,
Solberg, & Parker, 2010) to promote physical activity
(PA) and improve diet quality, evidence remains insufficient
for determining the efficacy of school-based interventions,
particularly those that can be broadly disseminated, in
improving these behaviors among underserved adolescents,
especially for those who are Black, in order to reduce
the high OW/OB prevalence (Barr-Anderson, Singleton,
Cotwright, Floyd, & Affuso, 2014; Kornet-van der Aa,
Altenburg, van Randeraad-van der Zee, & Chinapaw,
2017). Although targeting schools is important for reaching
these at-risk adolescents (Nordin et al., 2010), some
researchers are recommending that school-based interven-
tions also extend into the home to actively involve parents/
guardians (further referred to as parents) to help underserved
young adolescents increase their PA and diet quality (D. K.
Wilson, Van Horn, et al., 2011).
Background
In a review of the literature, we found five school-based
studies that focused on improving body mass index (BMI)
and included young adolescents in economically disadvan-
taged communities. Only two of the five significantly
improved BMI and BMI z-score with small-to-moderate
1
College of Nursing, Michigan State University, East Lansing, MI, USA
2
Department of Kinesiology, Michigan State University, East Lansing, MI,
USA
3
Nursing Department, Hope College, Holland, MI, USA
4
Department of Epidemiology and Biostatistics, Michigan State University,
East Lansing, MI, USA
5
Center for Human Growth and Development, University of Michigan,
Ann Arbor, MI, USA
6
Department of Biostatistics, Center for Computational Medicine and
Bioinformatics, University of Michigan, Ann Arbor, MI, USA
Corresponding Author:
Lorraine B. Robbins, PhD, RN, FNP-BC, FAAN, College of Nursing,
Michigan State University, Bott Building for Nursing Education and
Research Room #C245, 1355 Bogue Street East Lansing, East Lansing, MI
48824, USA.
Email: [email protected]
The Journal of School Nursing
1-14
ªThe Author(s) 2018
Article reuse guidelines:
sagepub.com/journals-permissions
DOI: 10.1177/1059840518791290
journals.sagepub.com/home/jsn

effect sizes ranging from 0.31 to 0.70 (Lazorick, Fang,
Hardison, & Crawford, 2015; Lubans, Morgan, Aguiar, &
Callister, 2011). The remaining three studies reported very
small effect sizes on BMI or BMI z-score ranging from
0.07 to 0.04 (Foster et al., 2008; Franckle et al., 2017;
Hollis et al., 2016). However, the two studies with signifi-
cant results had relatively smaller sample sizes than the
remaining three studies (N¼100, 362 vs. 1,150, 1,349,
219,762). Furthermore, one of the two studies, which was
conducted in the United States, did not include randomiza-
tion of the schools to intervention or control conditions and
provided US$20,000 dollars to each school for intervention-
related expenses; the other study, which was conducted out-
side the United States, involved boys only and did not blind
assessors to group assignment.
For the three studies that did not yield significant results,
intervention duration was 12 months in one (Hollis et al.,
2016) and 2 years in the remaining two studies (Foster et al.,
2008; Franckle et al., 2017), and parents were either not
involved or had minimal involvement (e.g., newsletters
about PA sent home; at school meetings, parents encouraged
to assist their children to engage in healthy behaviors). The
12-month intervention was theory based, but focused on PA
only; whereas the other two interventions were not theory
based and involved varied curricular and policy changes to
improve PA and diet quality.
For the two studies that had significant results, the inter-
ventions were theory based, focused on PA and diet quality,
andrangedindurationfrom14weeksto6months.Both
interventions had no parental involvement and included cur-
ricula delivered by teachers during the school day that
involved education, skill development (e.g., self-
monitoring, goal setting), and opportunities for PA. While
both studies demonstrated that school-based interventions
can be successful, altering the curricula during the school day
to promote PA and healthy eating may not be feasible in all
schools due to pressure perceived by administrators and
teachers to improve students’ academic performance (Beets
et al., 2016). Interventions that occur in conjunction with
schools, but take place after school, may be a necessary and
ideal solution for addressing these issues because most ado-
lescents attend school (D. K. Wilson, Van Horn, et al., 2011).
Although participation by adolescents in an after-school
program at their school to increase PA and healthy eating is
convenient and provides an opportunity for acquiring
knowledge and building skills, it may not be sufficient for
assisting them to adequately achieve both behavioral objec-
tives. Although active involvement of parents along with
their adolescents (Bradley et al., 2011) in interventions may
also be important, involving parents has been a challenge
(Smith, Wohlstetter, Kuzin, & De Pedro, 2011), indicating a
need to test novel approaches.
In a systematic review of PA and dietary mobile applica-
tions, Brannon and Cushing (2015) found that apps targeting
health promotion by focusing on improving both adolescent
PA and diet quality are sparse with limited incorporation of
strategies to strengthen theoretical constructs, such as social
support, that have already been identified as important pre-
dictors of positive behavior change. Another limitation is
that technology for promoting healthy behaviors is usually
designed for the individual who needs to change as opposed
to the one who can offer support for the process (Ferrer &
Ellis, 2017). Due to pervasive use among adults, social net-
working platforms, such as Facebook, may have the poten-
tial to address these limitations and bolster parents’ support
for their adolescents to make positive behavioral changes.
Despite the promise of this approach, we found no interven-
tion to empower parents via Facebook to assist their adoles-
cents with increasing PA and diet quality, indicating that the
capability of social networking for achieving this objective
remains basically untapped (Cavallo et al., 2014; Hammers-
ley, Jones, & Okely, 2016).
To address these issues, we conducted a pilot study to test
a 12-week, three-component Guys/Girls Opt for Activities
for Life (GOAL) intervention that involved parents via Face-
book, as an adjunct to a single parent–adolescent dyad meet-
ing and also an after-school club (2 days/week) for urban,
underserved adolescents. To our knowledge, no study
including an intervention combining these three components
has been conducted with parents and adolescents of low
socioeconomic and minority status. Based on this informa-
tion, the primary purpose of this study was 2-fold: (1) to
evaluate the feasibility and acceptability of our school- and
home-based intervention and (2) to examine the preliminary
efficacy of the intervention versus a control condition on
fifth- to seventh-grade adolescents’ accelerometer-
measured moderate-to-vigorous physical activity (MVPA);
diet quality; and psychosocial variables including motiva-
tion, self-efficacy, and perceived social support for PA and
healthy eating. A secondary aim was to explore any effect of
the intervention on adolescents’ percent body fat and BMI.
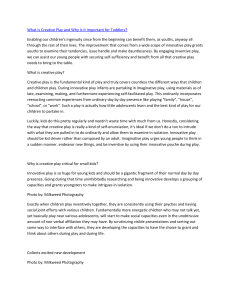
Theoretical Framework
The intervention was guided by self-determination theory
(SDT; Ryan & Deci, 2000) and the information–motiva-
tion–behavioral skills (IMB) model (Fisher, Fisher, Bryan,
& Misovich, 2002). The SDT identifies the following three
basic needs that promote intrinsic motivation to drive beha-
vior: competence (self-efficacy), autonomy (choice), and
relatedness (social support). The IMB model indicates that
making a positive change in behavior is increased when an
individual has information, motivation, and behavioral skills
for accomplishing the task. Self-efficacy (Fitzgerald, Heary,
Kelly, Nixon, & Shevlin, 2013), social support from others
(e.g., parents, peers, and instructors or teachers; Glozah &
Pevalin, 2015; Lytle et al., 2009), and motivation (Dwyer
et al., 2017; Huffman, Wilson, Van Horn, & Pate, 2017)
are related to MVPA and healthy eating among adolescents.
All three components of GOAL were designed to increase
2The Journal of School Nursing XX(X)

the latter three modifiable psychosocial variables among
adolescents, including motivation, self-efficacy, and
perceived social support for PA and healthy eating (see
Figure 1; Table 1).
Method
Study Design
The Michigan State University Biomedical Institutional
Review Board approved the study, and administrators pro-
vided approval to conduct it in their respective schools. A
pretest–posttest quasi-experimental design was used. After
adolescents completed baseline data collection, a statistician
not involved in the study randomly assigned one of the two
kindergarten to eighth-grade public schools located in the
same low-socioeconomic status (SES), large urban school
district in the Midwestern United States to receive the
GOAL intervention. The remaining school served as a con-
trol condition with participants receiving usual activities that
were similar to those of the intervention school.
Recruitment
All adolescents in the selected academic grades were called
to an assembly at each school so researchers could describe
the study protocol and invite them to participate. Adoles-
cents were told that, after baseline data were collected, their
school would be randomly assigned by a statistician to
receive either GOAL or usual school activities, and then
they would be contacted to hear the randomization status
of their school. The researchers distributed a packet contain-
ing study information, consent, and assent forms, and a
screening tool to determine eligibility to all adolescents.
Researchers told adolescents to share the packet of informa-
tion with their parents and to return the packets, including
completed forms indicating whether they are interested in
participating or not, to researchers present at their school
during the next 2 days. Researchers informed adolescents
that written parental consent and adolescent assent would
be required prior to participation.
Participants and Setting
Participants were included if they were 10–13 years of age;
in fifth to seventh grade; able to read, understand, and
speak English; agree to random assignment; available to
participate in GOAL, including after-school program 2
days/week, if offered at their school; and able to identify
one parent who is willing and able to serve as a support
person by (a) assisting the adolescent to attain adequate PA
and eat healthy, (b) participating with the adolescent in one
face-to-face meeting occurring during the first intervention
week, and (c) completing weekly healthy habit-forming
tasks to help the adolescent increase PA and healthy eating
and posting in a private Facebook group. Participants were
excluded if they had a mental or physical health condition
precluding safe participation or were involved in school or
community sports or other organized programs (e.g., dance
lessons) that involved MVPA and required participation
after school 4 or more days per week during the school
year. Thirty-nine adolescents and 38 parents in the inter-
vention school and 45 adolescents and 43 parents from the
control school enrolled (N¼81 dyads total). One twin in
each of three families was randomly selected for inclusion
in data analysis. A median sample size of 30 per group is
adequate for a pilot study (Billingham, Whitehead, &
Julious, 2013). With regard to overall student enrollment
in the selected grades in each school (n¼115 intervention,
n¼173 control), compared to the control school, the inter-
vention school had a lower percentage of female (59.5%vs.
41.7%), White (18.5%vs. 13.9%), and Hispanic students
(19.1%vs. 12.2%), and a higher percentage of Black
(41.0%vs. 62.6%) and disadvantaged students (66.5%vs.
75.7%; Michigan’s Center for Educational Performance
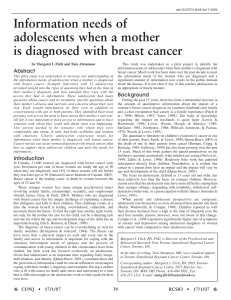
and Information, 2018). Figure 2 depicts the flow diagram
of participants.
Measures
Demographics. Each parent responded to survey questions
about the parent’s and adolescent’s age, sex, and race/ethni-
city; parent’s marital status and SES (employment,
Proximal
Outcomes
•Minutes of MVPA
(accelerometer-
measured)
•Diet quality
Distal
Outcomes
•BMI
•% body
fat
Demographics
•Age, sex,
race/ethnicity,
academic grade,
SES
Intervention - Information, Motivational Messages, & Behavioral
(IMB Model) Strategies underpinning the following 3 intervention
components delivered to increase three modifiable psychosocial
variables, including adolescents’ Self-Efficacy, Social Support,
and Motivation (SDT: Competence, Relatedness, & Autonomy):
1) After-school GOAL Club, including MVPA
& healthy eating and cooking skill development (targeting self-
efficacy, social support, and motivation)
2) Parent-adolescent dyad meeting (targeting self-efficacy, social
support, and motivation)
3) GOAL social networking app for parents (with their adolescent;
targeting self-efficacy, social support, and motivation)
Figure 1. Theoretical framework.
Robbins et al. 3

educational level, and annual family income); and adoles-
cent’s academic grade.
Minutes of MVPA. Minutes of MVPA were assessed via
ActiGraph GT3Xþ(Version 3.2.1), a triaxial acceler-
ometer (http://www.theactigraph.com) that is reliable and
valid for assessing MVPA (Ha¨nggi, Phillips, & Rowlands,
2013). Monitors were worn at the hip on an elastic belt and
were set to begin data collection at 5 a.m. on the day after
monitors were given to adolescents at school. To remind
adolescents to wear it (Trost, McIver, & Pate, 2005), each
received a text message (and/or phone call at home if
preferred) every morning. Monitors were returned to
school after the seventh day of data collection (Trost, Pate,
Freedson, Sallis, & Taylor, 2000). Data were collected in
raw mode and reintegrated into 15-s epochs (Evenson,
Catellier, Gill, Ondrak, & McMurray, 2008). The follow-
ingsegmentsofthedaywhenmost participants would be
asleep or not wearing their monitor were filtered out: 9
p.m.to7a.m.onweekdaysand9p.m.to11a.m.on
weekends (Catellier et al., 2005). Nonwear time (defined
as periods with at least 60 consecutive zeros) was
removed, allowing for 2-min disruptions up to 100
counts/min (Troiano et al., 2008). Participants with at least
480 min/day of wear time on at least 3 days, including 1
weekend day, were included in subsequent analysis
(Penpraze et al., 2006). Age appropriate cut points were
used to identify mean minutes per hour of MVPA via
ActiLife 6 (Version 6.13.2) software. MVPA was classi-
fied as 574 counts/15 s (Evenson et al., 2008).
Diet quality. At baseline and postintervention, adolescents
completed the web-based Automated Self-Administered
24-Hour (ASA24) Dietary Assessment Tool, which is
reported to be valid for 24-hr dietary recall (Subar et al.,
2012; Thompson et al., 2015). Using a laptop computer at
each time period, adolescents individually reported their
dietary intake for the previous day. Data with caloric intake
less than 600 kcal/day were removed (Automated Self-
Administered 24-Hour Dietary Assessment Tool: Reviewing
and Cleaning ASA24
®
Data, 2017). Based on the ASA24
results, a Healthy Eating Index (Guenther et al., 2014) was
computed (possible scores 0–100), indicating the degree to
which an individual meets dietary guidelines. Fruit intake
was scored from 0 (no fruit)to5(0.4 cup equivalents/
1,000 kcal) and vegetable intake was scored from 0 (no
vegetables)to5(1.1 cup equivalents/1,000 kcal).
BMI and percent body fat. Two research assistants (RAs)
measured each adolescent’s height and weight behind a pri-
vacy screen at school. Height without shoes was measured to
the nearest 0.10 cm with a Shorr Board (Weigh and Measure,
Table 1. Description of the Three Intervention Components and Weeks of Delivery.
Weeks Intervention Components
1Parent–Adolescent Dyad Meeting (120 min) conducted at adolescents’ school to assist parents in supporting adolescents’ MVPA and
healthy eating included:
Discussion of information, behavioral strategies to assist parents in helping their adolescent increase healthy eating and PA
Chef conducted healthy eating and cooking session and distributed bag of groceries to facilitate preparation of the
demonstrated recipe by dyads at home
2–12 After-school GOAL Club began for adolescents, including PA and healthy eating and cooking skill building (18 events; 2 days/week; not
offered during winter/spring school breaks or no-school days)
50-min PA session included:
5-min discussion of the week’s PA theme plus information and behavioral strategies that parents were receiving via
Facebook, followed by a motivational message;
5 min of warm-up/stretching;
20 min of sport skill building;
15 min of fun games or game to apply learned sports skills; and
5 min of cooldown/stretching.
50-min “hands on” healthy eating and cooking skill-building session included:
5-min discussion of the week’s healthy eating and cooking theme plus information and behavioral strategies that parents
are receiving via Facebook, followed by a motivational message
45 min involving small groups working at mobile kitchens to prepare a healthy beverage, snack, or meal and then sample
what they prepared
Facebook Participation included the following weekly healthy eating and PA habit-forming tasks to assist parents in helping their
adolescents with MVPA and healthy eating and cooking:
Post a comment or picture about the healthy recipe you selected to make with your adolescent or about a strategy that
you used to help your adolescent eat healthy
Post a comment or picture about the PA that you helped your adolescent engage in or a strategy that you used to help your
adolescent get PA
Note. MVPA ¼moderate-to-vigorous physical activity; PA ¼physical activity; GOAL ¼guys/girls opt for activities for life.
4The Journal of School Nursing XX(X)

LLC, Olney, MD). RAs asked adolescents as needed to
remove hair accessories or change hairstyles. If an adoles-
cent refused, RAs obtained the measurement but also mea-
sured hairdo height (using a small plastic ruler) and recorded
all information on the data collection form. With the ado-
lescent in light clothing and no shoes, weight in kilograms to
nearest 0.10 kg and percent body fat to the nearest 0.1%
were measured using a Foot-to-Foot Bioelectric Impedance
Scale (Tanita Corporation, Tokyo, Japan). Two measure-
ments were taken for height, weight, and percent body fat.
If differences between the two measurements were 0.5 cm
for height, 0.5 kg for weight, or 0.5%for percent body
fat, a third was taken. The two closest measures were
recorded on the data collection form and averaged. Adoles-
cent BMI for age and sex was determined using the online
SAS program for Centers for Disease Control and Preven-
tion (2015) Growth Charts. Healthy weight was defined as
<85th percentile, while OW/OB was defined as 85th per-
centile. Validity in percent body fat via bioelectric impe-
dance for adolescents has been demonstrated by
comparisons to dual-energy X-ray absorptiometry (Barreira,
Staiano, & Katzmarzyk, 2013), the latter of which is not
feasible in schools.
At baseline, parents were invited to their respective
schools for height and weight measures. The procedure
was similar to the one employed for adolescents. BMI
Enrollment
Randomized schools to Intervention and Control conditions
Analyzed (n=34 adolescents)
•Excluded 1 adolescent from analysis
due to 1 parent/guardian having twins
(1 adolescent twin randomly selected
for inclusion in analysis)
Analyzed (n=43 adolescents)
•Excluded 2 adolescents from analysis
due to 2 parents/guardians having twins
(1 adolescent twin from each family
randomly selected for inclusion in
analysis)
Analysis
Of 288 enrolled students, 252 (87.5%) present at schools during time of recruitment received study enrollment packets.
school 1 (n=101 received packets of 115 enrolled students)
school 2 (n=151 received packets of 173 enrolled students)
Returned Packets (n=163)
school 1 (n=67)
school 2 (n=96)
Enrolled
school 1 (n=39 adolescents; 38 parents/guardians)
school 2 (n=45 adolescents; 43 parents/guardians )
Baseline Data Collection
school 1 (n=39 adolescents; 38 parents/guardians)
school 2 (n=45 adolescents; 43 parents/guardians)
• Declined (n=22 in school 1; n=43
in school 2)
• Excluded - not meeting
inclusion/exclusion criteria (n=1 in
school 1; n=8 in school 2)
• Unable to participate - personal
reasons (n=5 in school 1; 0 in
school 2)
Allocated to intervention (n=39 adolescents;
n=38 parents/guardians)
Allocated to control (n= 45 adolescents; n=43
parents/guardians)
Allocation
Lost to follow-up (n=4 adolescents [2
relocated; 1 refused; 1 removed for
misbehavior]); n=35 adolescents
completed post-intervention measures
Lost to follow-up (n=0 adolescents);
n=45 adolescents completed post-
intervention measures
Post-Intervention
Figure 2. Participant flow diagram.
Robbins et al. 5
 6
7
8
9
10
11
12
13
14
6
7
8
9
10
11
12
13
14
1
/
14
100%