Aggressiveness of Care in Advanced NSCLC Patients: A Prospective Cohort Study
Telechargé par
teguig.kenza

Aggressiveness of Care in a Prospective Cohort
of Patients With Advanced NSCLC
Jennifer S. Temel, MD
1
Jessica McCannon, MD
2
Joseph A. Greer, PhD
3
Vicki A. Jackson, MD
4
Patricia Ostler, RN
1
William F. Pirl, MD
5
Thomas J. Lynch, MD
1
J. Andrew Billings, MD
4
1
Department of Hematology/Oncology, Massa-
chusetts General Hospital, Boston, Massachu-
setts.
2
Department of Internal Medicine, Massachu-
setts General Hospital, Boston, Massachusetts.
3
Department of Behavioral Medicine, Massachu-
setts General Hospital, Boston, Massachusetts.
4
Department of Palliative Care, Massachusetts
General Hospital, Boston, Massachusetts.
5
Department of Psychiatry/Psychooncology, Mas-
sachusetts General Hospital, Boston, Massachu-
setts.
BACKGROUND. Optimal end of life care of patients with terminal cancer is poorly
understood. In this study, the aggressiveness of care is described in a cohort of
patients with newly diagnosed advanced nonsmall-cell lung cancer (NSCLC).
METHODS. Patients within 8 weeks of diagnosis of stage IIIb (with effusions) or IV
NSCLC were enrolled in a study to examine the feasibility of involving palliative
care services early in the provision of cancer care. Participants received standard
oncology treatment and integrated palliative care. All patients were followed pro-
spectively to assess anticancer therapy usage, hospital admissions, hospice utili-
zation, and location of death.
RESULTS. At the time of analysis, 40/46 (87%) of enrolled patients had died, with
a median length of follow-up of 29.3 months. Aggressive care measures in the
final month of life included rates of anticancer therapy (40%), emergency depart-
ment visits (48%), and hospital admissions (50%). Sixty-five percent of patients
received hospice care before death, with a median length of stay of 16 days.
Patients with heightened baseline anxiety and mood symptoms were more likely
to receive anticancer therapy at the end of life compared with those without
such symptoms.
CONCLUSIONS. This study demonstrates the frequent use of aggressive measures
at the end of life among patients with advanced NSCLC in a tertiary care center,
as shown by the number of patients receiving anticancer therapy within 30 days
of death and brief utilization of hospice services. Further research is needed to
identify predictors of aggressive care and to develop interventions enhancing
decision-making at the end of life. Cancer 2008;113:826–33. 2008 American
Cancer Society.
KEYWORDS: end-of-life care, nonsmall-cell lung cancer, hospice care, chemother-
apy.
The quality of end of life (EOL) care is gaining increasing atten-
tion as a key measure of excellence in cancer care.
1–3
Several
consensus statements and surveys of patients, families, and clini-
cians have been published affirming the value of not simply
prolonging life but also enhancing the quality of the dying pro-
cess.
4-7
Some of the more common themes regarding patients’
wishes for EOL care include adequate pain and symptom manage-
ment, preparation for death, and control over place of death.
Advanced care planning and EOL decision-making are also salient
indicators of quality care.
8,9
Although medical professionals, patients, and families have
articulated priorities for excellent care at EOL, the extent to which
such standards are translating into actual practice remains unclear.
What EOL treatment choices are patients, families, and clinicians
making when confronted with a terminal diagnosis? Previous
This study was funded by an investigator-initiated
research grant from Amgen (to J.S.T.) and NCI-
sponsored grant R03CA128478 (to J.A.G.).
Portions of this study were presented in poster
format at the ASCO Annual Meeting, Chicago, Illi-
nois, June 2007.
Address for reprints: Jennifer S. Temel, MD,
Massachusetts General Hospital, Yawkey 7B, 55
Fruit St., Boston, MA 02114; Fax: (509) 561-
9096; E-mail: [email protected]
Received October 23, 2007; revision received
March 14, 2008; accepted March 18, 2008.
ª2008 American Cancer Society
DOI 10.1002/cncr.23620
Published online 10 July 2008 in Wiley InterScience (www.interscience.wiley.com).
826

research indicates a trend toward increasingly aggres-
sive care among patients with advanced cancer.
10
Potential metrics of aggressive care that researchers
have identified as amenable for administrative data
analysis include use of chemotherapy, hospital
admissions, length of stay in routine inpatient or
ICU beds, emergency department visits, and utiliza-
tion of hospice services.
11
To date, a limited number of studies have been
published regarding the medical service utilization
patterns of patients with advanced diseases. How-
ever, these studies uniformly reveal high rates of
chemotherapy usage and hospital admissions near
EOL.
10,12-14
In addition, whereas the percentage of
patients referred to hospice before death appears to
be on the rise, the length of stay in hospice is declin-
ing.
10,13,15
The majority of these studies describing
chemotherapy use and other aggressive measures at
EOL, however, have been retrospective case series,
providing a limited and potentially biased account of
services delivered only to patients who have died
during a specific timeframe. To obtain a more accu-
rate understanding of EOL care, prospective cohort
studies are needed to identify patients who are ter-
minal and subsequently follow them until the time
of death. Such cohort designs allow for more repre-
sentative subject enrollment and unbiased delinea-
tion of study time periods.
16
Given the lack of prospective data in this area
the decision-making and resulting treatment prac-
tices of patients with advanced cancer require further
explication. For example, although previous research
suggests that patients have higher quality deaths
when receiving hospice services and families report
better bereavement outcomes when hospice care is
delivered over an extended period of time, aggressive
treatment may interfere with early referral.
17-22
More
specifically, if greater numbers of patients are receiv-
ing chemotherapy in the last month of life, then it is
unreasonable to expect hospice referrals or length of
stay in hospice to increase with the current reimbur-
sement model for such care. Efforts to lengthen stay
in hospice that fail to address the inability of hospice
programs to pay for costly anticancer therapy will be
fruitless. We must, therefore, endeavor to understand
the current practices of care for advanced cancer
patients and to obtain accurate baseline data on the
aggressiveness of oncology treatment before develop-
ing and testing interventions to improve EOL care.
In this study, we describe the EOL care practices
of 46 patients with newly diagnosed, advanced
NSCLC followed throughout the course of disease
while receiving concurrent oncology and palliative
treatment at a large academic medical center. By
using previously defined indicators of quality EOL
care including chemotherapy, hospital, and hospice
utilization patterns,
11
we prospectively examined the
aggressiveness of cancer care these patients received
from the time of diagnosis of incurable disease.
MATERIALS AND METHODS
Patient Selection
As part of a study examining the feasibility of ambu-
latory palliative care early in cancer management,
patients with advanced NSCLC were prospectively
followed throughout the course of cancer care.
23
This
article presents a subset analysis of patients accrued
at Massachusetts General Hospital (MGH) in which
endpoints of anticancer treatment and other meas-
ures of aggressiveness in EOL care were examined.
The Dana-Farber/Partners Cancer Care Institutional
Review Board-approved the project protocol, and all
participants provided written informed consent
before the initiation of the study.
Patients within 8 weeks of diagnosis of ad-
vanced-stage NSCLC (stage IIIb with pleural or peri-
cardial effusion or stage IV) who had an Eastern
Cooperative Oncology Group (ECOG) performance
status (PS) of 0-1 and the ability to read and respond
to questions in English were eligible to participate in
the early palliative care trial. The treating oncologists
and members of the study team approached eligible
patients consecutively to request their participation
in the intervention. All patients received standard on-
cology treatment and integrated palliative care ser-
vices, which included meeting with the palliative
care team at least monthly during outpatient periods
and daily during inpatient admissions. Although the
oncologists were informed of patient enrollment in
the palliative care study, they were unaware of the
aims of this secondary analysis regarding aggressive-
ness of care at EOL.
Measures and Data Collection
Anticancer therapy administration
A board-certified oncologist collected information on
anticancer therapy from the electronic medical re-
cord (EMR). Specifically, data came from the EMR
Infusion Flow sheets, which contain information on
intravenously administered chemotherapy, including
names of medications and dates of administration.
Details regarding the prescription of oral agents (ie,
epidermal growth factor receptor tyrosine kinase
inhibitors) and the administration of chemotherapy
as part of a clinical trial were available in the EMR as
well.
Aggressiveness of Care in Advanced NSCLC/Temel et al 827
10970142, 2008, 4, Downloaded from https://acsjournals.onlinelibrary.wiley.com/doi/10.1002/cncr.23620 by Algeria Hinari NPL, Wiley Online Library on [13/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License

Emergency department visits and inpatient hospitalizations
Information on visits to the emergency department
(ED) was obtained from patients’ EMR notes, includ-
ing presentations to the emergency department at
both the host hospital as well as outside institutions,
which routinely notify the host hospital staff when
ED visits or inpatient admissions occur. For all hos-
pitalized patients the inpatient paper medical record
and electronic hospital discharge summaries were
reviewed to collect data on hospital length of stay,
admission to the intensive care unit, administration
of chemotherapy, and death in the hospital.
Hospice referral
Hospice referrals for ambulatory patients are mana-
ged and recorded by a nurse liaison, who maintains
a database of dates of service. Inpatient referrals
occur at the time of discharge and are recorded in
the electronic discharge summary. For both outpati-
ents and inpatients, dates of hospice referral were
confirmed in the clinical notes of the EMR.
Date and site of death
The MGH Thoracic Oncology Department maintains
a Death Registry, based on physician report, of the
date and location of death for all clinic patients. In
addition, dates of death were confirmed using the
Social Security Death Index.
Quality of life (QOL) and symptom assessment
Study participants completed several QOL and mood
assessments at the time of informed consent and
periodically during follow up. Briefly, the Functional
Assessment of Cancer Therapy – Lung (FACT-L) was
used to measure health-related QOL. Items are meas-
ured on a 5-point Likert-type scale, yielding a total
score of 132, with higher scores indicating better
physical, emotional, social, and functional well-
being. The Lung Cancer Subscale of the FACT-L
includes 7 items assessing symptoms specific to lung
cancer; scores less than 24 indicate clinically signifi-
cant impairment.
24
The Hospital Anxiety and Depres-
sion Scale (HADS) was used to assess mood and
anxiety symptoms. A score of 8 or greater on each
subscale of the HADS was the cutoff for identifying
patients with possible anxiety and depression based
on published guidelines.
24,25
The administration of
these questionnaires has been described elsewhere;
only the baseline scores were analyzed for this
study.
23
Statistical Analysis
Descriptive statistics were initially calculated to esti-
mate the frequencies, means, and standard devia-
tions of the study variables. Unadjusted bivariate
associations between baseline patient characteristics
and aggressiveness of care indicators were analyzed
using 2-sided Fisher exact tests.
RESULTS
Forty-six patients were accrued at MGH between De-
cember 2003 and June 2005. At the time of data anal-
yses 40 patients had died, and data regarding their
EOL care are presented. The majority of the sample
was female (63%), diagnosed with stage IV NSCLC
(92%), and of good performance status (78% PS 51).
Patient demographics are shown in Table 1. Median
length of follow-up for the entire cohort was 29.3
months.
Anticancer Therapy Utilization
Ten patients (25%) underwent radiation therapy as
their initial treatment before systemic therapy. Two
patients (5%) received chemotherapy (ie, carboplati-
num/paclitaxel, gefitinib) while hospitalized, whereas
the remainder were treated in the outpatient setting.
All 40 patients eventually received some form of sys-
temic therapy. First-line anticancer therapy included
a platinum-based doublet (with or without a third
agent) (73%), an oral epidermal growth factor tyro-
sine kinase inhibitor (EGFR-TKI) (17%), or a single
parenteral agent (10%). Because of failure of
response and/or toxic side effects, 60% of patients
received second-line therapy, 38% received third-line
therapy, and 18% received fourth-line or greater.
TABLE 1
Baseline Patient Characteristics
Variable No. of Patients, N540 Percentage of Patients
Median age [range] 66.5 [45-82] —
White race 40 100
Women 25 63
Performance status
08 20
131 78
21 2
Stage
IIIb 3 8
IV 37 92
Initial therapy
Chemotherapy 24 60
Oral EGFR-TKI 6 15
Radiation 10 25
EGFR-TKI indicates epidermal growth factor tyrosine kinase inhibitor.
828 CANCER August 15, 2008 / Volume 113 / Number 4
10970142, 2008, 4, Downloaded from https://acsjournals.onlinelibrary.wiley.com/doi/10.1002/cncr.23620 by Algeria Hinari NPL, Wiley Online Library on [13/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License

Anticancer Therapy and Other Aggressive
Measures at the End of Life
Table 2 details the trends in anticancer therapy and
other aggressive measures at EOL. A sizeable propor-
tion of patients (n 516, 40%) received anticancer
therapy within 30 days of death, 5 of whom were
started on a new regimen. Although the majority of
patients enrolled in hospice services (65%), some
continued with more aggressive medical care during
the last month of life including visits to the ED (48%)
as well as admissions to the hospital (50%). Average
length of stay in the hospital within 30 days of death
was 4.05 inpatient days (SD 55.34).
Approximately one-quarter of the sample (n 59,
23%) underwent anticancer treatment within 14 days
of death, none of whom simultaneously received
hospice services. Of these 9 patients, 3 had been
newly diagnosed and received only first-line antican-
cer therapy before their death. The other 6 patients
continued existing regimens (number of regimens
ranged from 2 to 4), with 5 patients receiving oral
EGFR-TKIs before their death. The average number
of days between the start of anticancer therapy and
death for the 9 patients was 43.78 (SD 535.52), and
the average number of days between the final dose
of anticancer therapy and death was 7.33 (SD 5
3.67). The last definitive imaging studies for 3 of the
9 patients were at diagnosis, whereas the remaining
6 had at least 1 follow-up scan within the final
month of life, all showing disease progression. These
6 patients all received routine screening (scans at
least every 2 months) while on therapy, throughout
the course of their disease. Finally, of these 9 patients
who underwent anticancer therapy within 14 days of
death, 6 were ultimately admitted to hospice ser-
vices, with an average length of stay of 5.83 days (SD
54.26).
Circumstances of Death
Most patients died at home with hospice care or in
an inpatient hospice facility (62%), although 25%
were in a hospital setting at the time of death (see
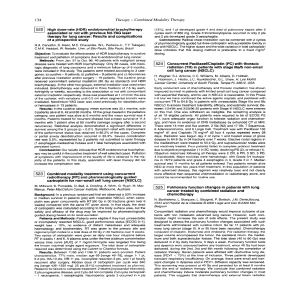
Table 3). For those patients who enrolled in hospice
care the median length of stay was 16 days, with
approximately one-third (31%) of patients receiving
services for less than 1 week. In contrast, 35% had a
length of stay in hospice of greater than 1 month, as
shown in Figure 1.
Bivariate Associations With Aggressive Care
At baseline, 32% (12/38) and 24% (9/38) of patients
reported clinically significant anxiety and depression
symptoms on the HADS, respectively, with 16% (6/
38) of the sample having comorbid anxiety and
depression. In addition, patients indicated impaired
QOL on the FACT-L (M 593.67, SD 516.30) and
Lung Cancer Subscale (M 519.21, SD 54.04).
To identify potential predictors of aggressive
care, exploratory bivariate analyses were conducted,
excluding newly diagnosed patients undergoing first-
line treatment only. Patients who received anticancer
therapy within 14 days of death were more likely to
have had elevated anxiety (67% vs 21%, P5.05, 2-
sided Fisher exact test) or depression scores (50% vs
11%, P5.05, 2-sided Fisher exact test) at the base-
line assessment, compared with those who did not
undergo such therapies in the final 2 weeks of life.
TABLE 2
Anticancer Therapy Use and Other Aggressive Measures
at the End of Life
Measure
M [SD; Range]
or N (%)
Average d between start of last anticancer therapy and death 109.60 [76.92; 2–342]
Average d between last anticancer therapy dose and death 49.72 [44.49; 2–169]
New anticancer therapy within 30 d of death 5 (13)
New or continued EGFR-TKI within 30 d of death 12 (30)
Any anticancer therapy within 30 d of death 16 (40)
Any anticancer therapy within 14 d of death 9 (23)
Any anticancer therapy within 7 d of death 6 (15)
Emergency department visit within 30 d of death 19 (48)
>1 emergency department visit within 30 d of death 4 (10)
Hospital admission within 30 d of death 20 (50)
>1 hospital admission within 30 d of death 5 (13)
Average number of inpatient d within 30 d of death 4.05 [5.34; 0–22]
Admission to the ICU within 30 d of death 1 (2)
No admission to hospice prior to death 14 (35)
M indicates mean; SD, standard deviation; d, days; EGFR-TKI, epidermal growth factor tyrosine
kinase inhibitor; ICU, intensive care unit.
TABLE 3
Circumstances of Death
Circumstances No. (%)
Location of death
Home 19 (47)
Nursing home or rehabilitation center 2 (5)
Inpatient hospice 6 (15)
Hospital facility 10 (25)
Unknown 3 (8)
Services prior to death
Hospice 26 (65)
None 10 (25)
Unknown 4 (10)
Length of stay in hospice
Mean d [SD] 30.27 [33.85]
Median d {range} 16.00 {2–132}
d indicates days; SD, standard deviation from the mean.
Aggressiveness of Care in Advanced NSCLC/Temel et al 829
10970142, 2008, 4, Downloaded from https://acsjournals.onlinelibrary.wiley.com/doi/10.1002/cncr.23620 by Algeria Hinari NPL, Wiley Online Library on [13/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License

No other patient characteristics, mood symptoms, or
QOL indicators significantly related the use of
aggressive measures at EOL, although these analyses
were limited by the small sample size.
DISCUSSION
In this prospective study from presentation to death
of newly diagnosed patients with stage IIIb or IV
NSCLC we focused on previously described measures
of ‘aggressive’ care, including initiation or continua-
tion of anticancer therapy within 30 days of death,
high rates of visits to the emergency department or
admissions to the hospital in the last month of life,
and hospice utilization and length of stay. Findings
from the present study reveal greater anticancer ther-
apy usage at the EOL and shorter length of stay on
hospice than in previous studies.
10,12,13
For example,
Earle et al conducted a case series analyzing Medi-
care claims of patients who died within 1 year of
diagnosis of lung, breast, colorectal, or other gastro-
intestinal cancers, reporting that 5.7% of patients
initiated new chemotherapy within 30 days of death
and 18.5% received chemotherapy within 14 days of
death for claims processed in 1996.
11
In contrast, we
observed even higher rates of anticancer therapy
usage (13% and 23%, respectively) during the final
weeks of life in a homogeneous sample of patients
with advanced NSCLC. Moreover, 40% of our patients
received either new or continued anticancer within
30 days of death compared with previous trials’ rates
of 11%, 26%, and 33%.
13,26,27
With regard to adminis-
tration of chemotherapy at EOL, the current climate
of oncology care for patients with late-stage lung
cancer is arguably an aggressive one.
The widespread use of anticancer therapy in
patients with advanced NSCLC is noteworthy given
the incurable nature of the disease and poor long-
term prognosis. The benefits of anticancer therapy
for metastatic NSCLC are quite modest, with recent
studies confirming the prolongation of median sur-
vival by only approximately 2 months using first-line
therapy.
28
All of the patients in our sample received
some form of first-line anticancer therapy. In
addition, 60% of patients in this sample received sec-
ond-line therapy and more than one-third received
third-line therapy, despite these agents having a dis-
appointing response rate of approximately 10%.
29–33
Although an additional 30% to 50% of patients trea-
ted with second-line anticancer therapy may have
stable disease, the median progression-free survival
remains low, at close to 2 months.
31,34
Therefore, the
benefits of second-line chemotherapy are usually
small and short-lived. A subset of patients in our
sample (18%) even received fourth-line therapy or
greater, although there is no FDA-indicated treat-
ment for such care.
Continuing multiple lines of anticancer therapy
at EOL is likely related to the availability of novel
oral agents, which may be less toxic and more easily
administered than intravenous infusion therapy. Of
the patients in our sample who received anticancer
therapy in the final month of life, most were pre-
scribed an oral EGFR-TKI (12/16 or 75%). Although
the FDA-approved oral EGFR-TKIs for advanced
NSCLC are less toxic than standard cytotoxic chemo-
therapy, they nonetheless have some side effects,
including rash and diarrhea.
32,35
The development of
these newer anticancer therapies allows for multiple
lines of chemotherapy and likely contributes to the
use of chemotherapy close to death, especially for
patients with such short life expectancy.
In addition to potential improvements in overall
survival, oncologists administer anticancer therapy to
alleviate symptom burden and for palliation. Multiple
studies have demonstrated that chemotherapy can
reduce symptoms in patients with advanced NSCLC.
For example, pain, cough, and fatigue have been
shown to improve with chemotherapy compared
with best supportive care.
33,36–39
The relationship
between chemotherapy and QOL is somewhat less
clear, namely because of the complex nature of QOL
and the difficulties in assessing it over time in an ill
patient population.
40
QOL is a multidimensional
construct that includes not only symptom burden,
but also social, emotional, functional, and spiritual
well-being. Although chemotherapy clearly impacts
symptoms and possibly functional well-being,
demonstrating improvements in social and emo-
tional well-being is more challenging, as those
domains are impacted by a variety of patient factors
other than anticancer therapy. Notably, a large, well-
designed, randomized study comparing chemother-
FIGURE 1. Length of stay in hospice before death.
830 CANCER August 15, 2008 / Volume 113 / Number 4
10970142, 2008, 4, Downloaded from https://acsjournals.onlinelibrary.wiley.com/doi/10.1002/cncr.23620 by Algeria Hinari NPL, Wiley Online Library on [13/08/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
 6
7
8
6
7
8
1
/
8
100%