167
CMDT 2022
REFRACTIVE ERRORS
Refractive error is the most common cause of reduced
clarity of vision (visual acuity).
Use of a pinhole will overcome most refractive errors
and thus allows their identification as a cause of reduced
visual acuity. Refractive error can be treated with glasses,
contact lenses, or surgery.
»Treatment
A. Contact Lenses
An estimated 40.9 million US adults wear contact lenses,
mostly for correction of refractive errors, though decorative-
colored contact lenses are used.
The major risk from contact lens wear is corneal infec-
tion, potentially a blinding condition. Such infections
occur more often with soft lenses, particularly extended
wear, for which there is at least a fivefold increase in risk of
corneal infection compared with daily wear. Decorative
contact lenses have a high prevalence of microbial con-
tamination. Contact lens wearers should be made aware of
the risks they face and ways to minimize them, such as
avoiding overnight wear or use of lenses past their replace-
ment date and maintaining meticulous lens hygiene,
including not using tap water or saliva for lens cleaning.
Contact lenses should be removed whenever there is ocular
discomfort or redness.
Razmaria AA. JAMA patient page. Proper care of contact lenses.
JAMA. 2015;314:1534. [PMID: 26462011]
B. Surgery
Various surgical techniques are available to reduce refrac-
tive errors, particularly nearsightedness. Laser corneal
refractive surgery reshapes the middle layer (stroma) of the
cornea with an excimer laser. Other refractive surgery
techniques are extraction of the clear crystalline lens with
insertion of a single vision, multifocal, or accommodative
intraocular lens as occurs after cataract extraction; inser-
tion of an intraocular lens without removal of the crystal-
line lens (phakic intraocular lens); intrastromal corneal
ring segments (INTACS); collagen cross-linking; laser
thermal keratoplasty; and conductive keratoplasty (CK).
Wilkinson JM et al. Refractive eye surgery: helping patients make
informed decisions about LASIK. Am Fam Physician. 2017;95:
637. [PMID: 28671403]
C. Reduction of Rate of Progression
of Nearsightedness
The rate at which nearsightedness progresses can be reduced
by topical atropine and pirenzepine, a selective muscarinic
antagonist; rigid contact lens wear during sleep (orthokera-
tology); and various types of soft contact lenses and specta-
cles, but their long-term efficacy and safety are uncertain.
»When to Refer
Any contact lens wearer with an acute painful red eye must
be referred emergently for ophthalmologic evaluation.
DISORDERS OF THE LIDS &
LACRIMAL APPARATUS
1. Hodolum
Hordeolum is an acute infection that is commonly due to
Staphylococcus aureus. It is characterized by a localized red,
swollen, acutely tender area on the upper or lower lid.
Internal hordeolum is a meibomian gland abscess that usu-
ally points onto the conjunctival surface of the lid; external
hordeolum, or stye, is usually smaller and on the lid margin
and is an abscess of the gland of Zeis.
Warm compresses are helpful. Incision may be indi-
cated if resolution does not begin within 48 hours. An
antibiotic ointment (bacitracin or erythromycin) applied to
the lid every 3 hours may be beneficial during the acute
stage. Internal hordeolum may lead to generalized cellulitis
of the lid.
2. Chlzion
Chalazion is a common granulomatous inflammation of a
meibomian gland that may follow an internal hordeolum.
It is characterized by a hard, nontender swelling on the
7
Jacque L. Duncan, MD
Neeti B. Parikh, MD
Gerami D. Seitzman, MD
Disorders of the
Eyes & Lids
CMDT22_Ch07_p0167-p0200.indd 167 29/06/21 8:31 PM

CHapter 7
168 CMDT 2022
upper or lower lid with redness and swelling of the adjacent
conjunctiva. Initial treatment is with warm compresses. If reso-
lution has not occurred by 2–3 weeks, incision and curettage is
indicated. Corticosteroid injection may also be effective.
3. Blhiis
Blepharitis is a common chronic bilateral inflammatory
condition of the lid margins. Anterior blepharitis involves
the lid skin, eyelashes, and associated glands. It may be
ulcerative because of infection by staphylococci, or sebor-
rheic in association with seborrhea of the scalp, brows, and
ears. Posterior blepharitis results from inflammation of the
meibomian glands. There may be bacterial infection, par-
ticularly with staphylococci, or primary glandular dysfunc-
tion, which is strongly associated with acne rosacea.
»Clinical Findings
Symptoms are irritation, burning, and itching. In anterior
blepharitis, the eyes are “red-rimmed” and scales or col-
lerettes can be seen clinging to the lashes. In posterior
blepharitis, the lid margins are hyperemic with telangiecta-
sias, and the meibomian glands and their orifices are
inflamed. The lid margin is frequently rolled inward to
produce a mild entropion, and the tear film may be frothy
or abnormally greasy.
Blepharitis is a common cause of recurrent conjunctivi-
tis. Both anterior and, especially, posterior blepharitis may
be complicated by hordeola or chalazia; abnormal lid or
lash positions, producing trichiasis; epithelial keratitis of
the lower third of the cornea; marginal corneal infiltrates;
and inferior corneal vascularization and thinning.
»Treatment
Anterior blepharitis is usually controlled by eyelid hygiene.
Warm compresses help soften the scales and warm the mei-
bomian gland secretions. Eyelid cleansing can be achieved
by gentle eyelid massage and lid scrubs with baby shampoo
or 0.01% hypochlorous acid. In acute exacerbations, an
antibiotic eye ointment, such as bacitracin or erythromycin,
is applied daily to the lid margins.
Mild posterior blepharitis may be controlled with regu-
lar meibomian gland expression and warm compresses.
Inflammation of the conjunctiva and cornea is treated with
long-term low-dose oral antibiotic therapy, eg, tetracycline
(250 mg twice daily for 2–4 weeks), doxycycline (100 mg
daily for 2–4 weeks), minocycline (50–100 mg daily for
2–4 weeks) erythromycin (250 mg three times daily for
2–4 weeks), or azithromycin (500 mg daily for 3 days in three
cycles with 7-day intervals). Short-term (5–7 days) topical
corticosteroids, eg, prednisolone, 0.125% twice daily, may
also be indicated. Topical therapy with antibiotics, such as
ciprofloxacin 0.3% ophthalmic solution twice daily, may be
helpful but should be restricted to short courses of 5–7 days.
Amescua G et al; American Academy of Ophthalmology Pre-
ferred Practice Pattern Cornea and External Disease Panel.
Blepharitis Preferred Practice Pattern®. Ophthalmology.
2019;126:P56. [PMID: 30366800]
4. enoion & ecoion
Entropion (inward turning of usually the lower lid) occurs occa-
sionally in older people as a result of degeneration of the lid
fascia or may follow extensive scarring of the conjunctiva and
tarsus. Surgery is indicated if the lashes rub on the cornea. Botu-
linum toxin injections may also be used for temporary correc-
tion of the involutional lower lid entropion of older people.
Ectropion (outward turning of the lower lid) is common
with advanced age. Surgery is indicated if there is excessive
tearing, exposure keratitis, or a cosmetic problem.
5. tumos
Lid tumors are usually benign. Basal cell carcinoma is the
most common malignant tumor. Squamous cell carcinoma,
meibomian gland carcinoma, and malignant melanoma
also occur. Surgery for any lesion involving the lid margin
should be performed by an ophthalmologist or suitably
trained plastic surgeon to avoid deformity of the lid. Histo-
pathologic examination of eyelid tumors should be routine,
since 2% of lesions thought to be benign clinically are found
to be malignant. Medications such as vismodegib (an oral
inhibitor of the hedgehog pathway), imiquimod (an immu-
nomodulator), and 5-fluorouracil occasionally are used
instead of or as an adjunct to surgery for some basal and
squamous cell carcinomas.
6. Dcyocysiis
Dacryocystitis is infection of the lacrimal sac usually due to
congenital or acquired obstruction of the nasolacrimal
system. It may be acute or chronic and occurs most often
in infants and in persons over 40 years. It is usually unilat-
eral. Infection is typically with S aureus and streptococci in
acute dacryocystitis and Staphylococcus epidermidis, strep-
tococci, or gram-negative bacilli in chronic dacryocystitis.
Acute dacryocystitis is characterized by pain, swelling,
tenderness, and redness in the tear sac area; purulent mate-
rial may be expressed. In chronic dacryocystitis, tearing and
discharge are the principal signs, and mucus or pus may
also be expressed.
Acute dacryocystitis responds well to systemic antibi-
otic therapy. To relieve the underlying obstruction, surgery
is usually done electively but may be performed urgently in
acute cases. The chronic form may be kept latent with sys-
temic antibiotics, but relief of the obstruction is the only
cure. In adults, the standard procedure is dacryocystorhi-
nostomy, which involves surgical exploration of the lacri-
mal sac and formation of a fistula into the nasal cavity and,
if necessary, supplemented by nasolacrimal intubation.
Congenital nasolacrimal duct obstruction is common
and often resolves spontaneously. It can be treated by prob-
ing the nasolacrimal system, supplemented by nasolacrimal
intubation or balloon catheter dilation, if necessary; dac-
ryocystorhinostomy is rarely required.
CONJUNCTIVITIS
Conjunctivitis is inflammation of the mucous membrane
that lines the surface of the eyeball and inner eyelids. It may
be acute or chronic. Most cases are due to viral or bacterial
CMDT22_Ch07_p0167-p0200.indd 168 29/06/21 8:31 PM

DISOrDerS OF tHe eYeS & LIDS 169
CMDT 2022
(including gonococcal and chlamydial) infection. Other
causes include keratoconjunctivitis sicca, allergy, chemical
irritants, and trauma. The mode of transmission of infec-
tious conjunctivitis is usually via direct contact of contami-
nated fingers or objects to the fellow eye or to other
persons. It may also be spread through respiratory secre-
tions or contaminated eye drops.
Conjunctivitis must be differentiated from acute uve-
itis, acute glaucoma, and corneal disorders (Table 7–1).
1. Vil Conjunciviis
Adenovirus is the most common cause of viral conjunctivi-
tis. There is usually sequential bilateral disease with copious
watery discharge and a follicular conjunctivitis. Infection
spreads easily. Epidemic keratoconjunctivitis, which may
result in decreased vision from corneal subepithelial infil-
trates, is usually caused by adenovirus types 8, 19, and 37.
The active viral conjunctivitis lasts up to 2 weeks, with the
immune-mediated keratitis occurring later. Infection with
adenovirus types 3, 4, 7, and 11 is typically associated with
pharyngitis, fever, malaise, and preauricular adenopathy
(pharyngoconjunctival fever). The disease usually lasts
10 days. Contagious acute hemorrhagic conjunctivitis (see
Chapter 32) may be caused by enterovirus 70 or coxsackie-
virus A24. Viral conjunctivitis from herpes simplex virus
(HSV) is typically unilateral and may be associated with lid
vesicles.
Except for HSV infection for which treatment with
topical (eg, ganciclovir 0.15% gel) and/or systemic (eg, oral
acyclovir, valacyclovir) antivirals is recommended
(Table 32–1), there is no specific treatment for contagious
viral conjunctivitis. Artificial tears and cold compresses
may help reduce discomfort. The use of topical antibiotics
and steroids in the acute infection is discouraged. Frequent
hand and linen hygiene is encouraged to minimize spread.
Varu DM et al; American Academy of Ophthalmology Preferred
Practice Pattern Cornea and External Disease Panel. Con-
junctivitis Preferred Practice Pattern®. Ophthalmology. 2019;
126:P94. [PMID: 30366797]
2. Bcil Conjunciviis
The organisms isolated most commonly in bacterial con-
junctivitis are staphylococci, including methicillin-resistant
S aureus (MRSA); streptococci, particularly Streptococcus
pneumoniae;Haemophilus species; Pseudomonas; and
Moraxella. All may produce purulent discharge and eyelid
matting. Blurring of vision and discomfort are mild. In
severe (hyperpurulent) cases, examination of stained con-
junctival scrapings and cultures is recommended, particu-
larly to identify gonococcal infection that requires emergent
treatment.
The disease is usually self-limited, lasting about
10–14 days if untreated. Most topical antibiotics hasten
clinical remission. This infection is typically self-limited,
and no topical antibiotic has proven superiority over another.
A. Gonococcal Conjunctivitis
Gonococcal conjunctivitis, usually acquired through contact
with infected genital secretions, typically causes copious
purulent discharge. It is an ophthalmologic emergency
because corneal involvement may rapidly lead to perfora-
tion. The diagnosis should be confirmed by stained smear
and culture of the discharge. Systemic treatment is required
with a single 1-g dose of intramuscular ceftriaxone plus
azithromycin 1000 mg orally (see Chapter 33). Fluoroqui-
nolone resistance is common. Eye irrigation with saline may
promote resolution of conjunctivitis. Topical antibiotics
such as erythromycin and bacitracin may be added. Other
sexually transmitted diseases, including chlamydiosis,
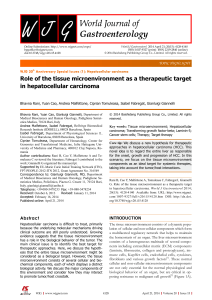
Table 7–1. The inflamed eye: differential diagnosis of common causes.
acu Conjunciviis
acu anio Uviis
(Iiis)
acu angl-Closu
Glucom
Conl tum o
Infcion
Incidence Extremely common CommonUncommonCommon
Discharge Moderate to copious Watery or purulentNoneNone
Vision No effect on vision Usually blurredMarkedly blurredOften blurred
Pain Mild Moderate to severeSevereModerate
Conjunctival injection Diffuse Mainly circumcornealMainly circumcornealMainly circumcorneal
Cornea Clear Clarity change related toCloudyUsually clear
cause
Pupil size Normal Normal or smallModerately dilatedSmall
Pupillary light response Normal NormalNonePoor
Intraocular pressure Normal Usually normal but may
be elevated
NormalMarkedly elevated
Smear Causative organisms Organisms found only inNo organismsNo organisms
corneal infection
CMDT22_Ch07_p0167-p0200.indd 169 29/06/21 8:31 PM

CHapter 7
170 CMDT 2022
syphilis, and HIV infection, should be considered. Routine
treatment for chlamydial infection is recommended.
B. Chlamydial Keratoconjunctivitis
1. Trachoma—Trachoma is the most common infectious
cause of blindness worldwide, with approximately 40 million
people affected and 1.2 million blind. Recurrent episodes
of infection in childhood manifest as bilateral follicular
conjunctivitis, epithelial keratitis, and corneal vasculariza-
tion (pannus). Scarring (cicatrization) of the tarsal con-
junctiva leads to entropion and trichiasis in adulthood with
secondary central corneal scarring.
Immunologic tests or polymerase chain reaction (PCR)
on conjunctival samples will confirm the diagnosis but
treatment should be started on the basis of clinical find-
ings. A single 1-g dose of oral azithromycin is the preferred
drug for mass treatment campaigns. Improvements in
hygiene and living conditions probably have contributed
more to the marked reduction in the prevalence of tra-
choma during the past 30 years. Local treatment is not
necessary. Surgical treatment includes correction of lid
deformities and corneal transplantation.
Godwin W et al. Trachoma prevalence after discontinuation of
mass azithromycin distribution. J Infect Dis. 2020;221:S519.
[PMID: 32052842]
2. Inclusion conjunctivitis—The eye becomes infected
after contact with genital secretions infected with chla-
mydia. The disease starts with acute redness, discharge,
and irritation. Examination shows follicular conjunctivitis
with mild keratitis. A nontender preauricular lymph node
can often be palpated. Healing usually leaves no sequelae.
Diagnosis can be rapidly confirmed by immunologic tests
or PCR on conjunctival samples. Treatment is with a single
dose of azithromycin, 1 g orally. All cases should be
assessed for genital tract infection and other sexually trans-
mitted diseases.
3. Dy eys
Dry eye, a common and chronic disorder, is an umbrella
term that describes a condition of tear film instability
and associated ocular and visual complaints. Dry eye is
more common in women than men and increases with
age. Hypofunction of the lacrimal glands, causing loss of
the aqueous component of tears (keratoconjunctivitis
sicca), may be due to aging, hereditary disorders, sys-
temic disease (eg, Sjögren syndrome), or systemic drugs.
Excessive evaporation of tears may be due to environ-
mental factors (eg, excessive screen time, windy climate)
or abnormalities of the lipid component of the tear
film, as in blepharitis. Mucin deficiency may be due to
vitamin A deficiency or conjunctival scarring from tra-
choma, Stevens-Johnson syndrome, mucous membrane
pemphigoid, graft-versus-host disease, chemical burns, or
topical drug toxicity.
»Clinical Findings
The patient complains of dryness, redness, foreign body
sensation, and variable vision. In severe cases, there is per-
sistent marked discomfort, with photophobia, difficulty in
moving the lids, and excessive mucus secretion. In many
cases, gross inspection reveals no abnormality, but on slit-
lamp examination there are abnormalities of tear film sta-
bility and reduced tear volume. In more severe cases,
damaged corneal and conjunctival cells stain with fluores-
cein and lissamine green. In the most severe cases, there is
marked conjunctival injection, mucoid discharge, loss of
the normal conjunctival and corneal luster, and epithelial
keratopathy that stains with fluorescein and may progress
to frank ulceration. The Schirmer test, which measures the
rate of production of the aqueous component of tears, may
be helpful.
»Treatment
Aqueous deficiency can be treated with artificial tears
drops or ointments. The simplest preparations are physio-
logic (0.9%) or hypo-osmotic (0.45%) solutions of sodium
chloride, which can be used as frequently as every half-
hour, but in most cases are needed only three or four times
a day. More prolonged duration of action can be achieved
with drop preparations containing a mucomimetic such as
hydroxypropyl methylcellulose (HPMC) or carboxymeth-
ylcelluose (carmellose). If there is tenacious mucus, muco-
lytic agents (eg, acetylcysteine 10% or 20%, 1 drop six times
daily) may be helpful.
Artificial tear preparations are generally safe and, in
most cases, are used three or four times a day. However,
preservatives included in some preparations to maintain
sterility are potentially toxic and allergenic and may cause
ocular surface toxicity in frequent users. Such reactions
may be misinterpreted as a worsening of the dry eye state
requiring more frequent use of the artificial tears and lead-
ing in turn to further deterioration, rather than being rec-
ognized as a need to change to a preservative-free
preparation. Preservative-free preparations are recom-
mended for any frequency of use greater than four times a
day. Eye drops claiming to “get the red out” are not recom-
mended as they cause toxicity and rebound hyperemia
with prolonged use.
Dry eye is considered an inflammatory ocular surface
disease. Accordingly, disease modification may require
episodic treatment with low potency corticosteroid drops.
All patients using topical corticosteroids should have their
intraocular pressure monitored by eye care professionals.
Corticosteroid-sparing anti-inflammatory drops such as
the calcineurin inhibitor cyclosporine 0.05% ophthalmic
emulsion (Restasis) and the integrin antagonist lifitegrast
5% are commonly used with no universal consensus of
efficacy. Lacrimal punctal occlusion by canalicular plugs or
cautery is useful in severe cases.
Blepharitis is treated as described above.
de Paiva CS et al. Topical cyclosporine A therapy for dry eye syn-
drome. Cochrane Database Syst Rev. 2019;9:CD010051.
[PMID: 31517988]
CMDT22_Ch07_p0167-p0200.indd 170 29/06/21 8:31 PM

DISOrDerS OF tHe eYeS & LIDS 171
CMDT 2022
Gonzales JA. . .Seitzman GD et al. Ocular clinical signs and diag-
nostic tests most compatible with keratoconjunctivitis sicca: a
latent class approach. Cornea. 2020;39:1013. [PMID: 32251167]
4. allgic ey Diss
Allergic eye disease is common and takes a number of dif-
ferent forms but all are expressions of atopy, which may
also manifest as atopic asthma, atopic dermatitis, or allergic
rhinitis.
»Clinical Findings
Symptoms include itching, tearing, redness, stringy dis-
charge, and occasionally, photophobia and visual loss.
Allergic conjunctivitis is common. It may be seasonal
(hay fever), developing usually during the spring or sum-
mer, or perennial. Clinical signs include conjunctival
hyperemia and edema (chemosis), the latter at times being
marked and sudden in onset. Vernal keratoconjunctivitis
also tends to occur in late childhood and early adulthood.
It is usually seasonal, with a predilection for the spring.
Large “cobblestone” papillae are noted on the upper tarsal
conjunctiva. There may be follicles at the limbus. Atopic
keratoconjunctivitis is a more chronic disorder of adult-
hood. Both the upper and the lower tarsal conjunctivas
exhibit a papillary conjunctivitis. Severe cases demonstrate
conjunctival fibrosis, resulting in forniceal shortening and
entropion with trichiasis. Corneal involvement, including
refractory ulceration, is frequent during exacerbations of
both vernal and severe atopic keratoconjunctivitis. The lat-
ter may be complicated by herpes simplex keratitis.
»Treatment
A. Mild and Moderately Severe
Allergic Eye Disease
Topical anti-inflammatory agents include mast cell stabiliz-
ers and antihistamines (Table 7–2). Mast cell stabilization
takes longer to act than antihistamines but can be useful
for prophylaxis. Topical vasoconstrictors, such as ephed-
rine, naphazoline, tetrahydrozoline, and phenylephrine,
alone or in combination with antihistamines, are available
as over-the-counter medications and not typically used
because of limited efficacy, rebound hyperemia, and fol-
licular conjunctivitis. Systemic antihistamines (eg, lorata-
dine 10 mg orally daily) may be useful in prolonged atopic
keratoconjunctivitis. In allergic conjunctivitis, specific
allergens may be avoidable.
B. Acute Exacerbations and
Severe Allergic Eye Disease
Topical corticosteroids (Table 7–2) are essential to control
acute exacerbations of both vernal and atopic keratocon-
junctivitis. Corticosteroid-induced side effects should be
monitored by eye care professionals and include cataracts,
glaucoma, and exacerbation of herpes simplex keratitis.
The lowest potency corticosteroid that controls ocular
inflammation should be used. Topical cyclosporine or
tacrolimus is also effective. Systemic corticosteroid or
other immunosuppressant therapy may be required in
severe atopic keratoconjunctivitis.
Beck KM, Seitzman GD et al. Ocular co-morbidities of atopic
dermatitis. part I: associated ocular diseases. Am J Clin
Dermatol. 2019;20:797. [PMID: 31359350]
Beck KM, Seitzman GD et al. Ocular co-morbidities of atopic
dermatitis. part II: ocular disease secondary to treatments.
Am J Clin Dermatol. 2019;20:807. [PMID: 31352589]
PINGUECULA & PTERYGIUM
Pinguecula is a yellowish, elevated conjunctival nodule in
the area of the palpebral fissure. It is common in persons
over age 35 years. Pterygium is a fleshy, triangular
encroachment of the conjunctiva onto the cornea and is
usually associated with prolonged exposure to wind, sun,
sand, and dust. Pinguecula and pterygium are often bilat-
eral and occur more frequently on the nasal side of the
conjunctiva.
Pingueculae rarely grow but may become inflamed
(pingueculitis). Pterygia become inflamed and may grow.
Treatment is rarely required for inflammation of pinguec-
ula or pterygium, and artificial tears are often beneficial.
The indications for excision of pterygium are growth
that threatens vision by encroaching on the visual axis,
marked induced astigmatism, or severe ocular irritation.
CORNEAL ULCER
Corneal ulcers are most commonly due to infection by
bacteria, viruses, fungi, or amoebas. Noninfectious
causes—all of which may be complicated by infection—
include neurotrophic keratitis (resulting from loss of cor-
neal sensation), exposure keratitis (due to inadequate lid
closure), severe dry eye, severe allergic eye disease, and
inflammatory disorders that may be purely ocular or part
of a systemic vasculitis. Delayed or ineffective treatment of
corneal ulceration may lead to devastating consequences
with corneal scarring and rarely intraocular infection.
Prompt referral is essential.
Patients complain of pain, photophobia, tearing, and
reduced vision. The conjunctiva is injected, and there may
be purulent or watery discharge. The corneal appearance
varies according to the underlying cause.
»When to Refer
Any patient with an acute painful red eye and corneal
abnormality should be referred emergently to an ophthal-
mologist. Contact lens wearers with acute eye pain, redness,
and decreased vision should be referred immediately.
INFECTIOUS KERATITIS
1. Bcil Kiis
Risk factors for bacterial keratitis include contact lens
wear—especially overnight wear—and corneal trauma,
including refractive surgery. The pathogens most commonly
isolated are staphylococci, including MRSA; streptococci;
CMDT22_Ch07_p0167-p0200.indd 171 29/06/21 8:31 PM
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
1
/
35
100%