Deep pelvic endometriosis: a radiologist’s
guide to key imaging features with clinical
and histopathologic review
Ayeh Darvishzadeh ,
1
Wendaline McEachern,
2
Thomas K. Lee,
3
Priya Bhosale,
4
Ali Shirkhoda,
1
Christine Menias,
5
Chandana Lall
1
1
Department of Radiology, University of California Irvine School of Medicine, 1001 Health Sciences Road, Irvine, CA 92617, USA
2
Department of Radiology, Mayo Clinic, Rochester, MN, USA
3
Department of Pathology, University of California Irvine School of Medicine, Irvine, CA, USA
4
Division of Diagnostic Imaging, UT MD Anderson Cancer Center, Houston, TX, USA
5
Department of Radiology, Mayo Clinic, Phoenix, AZ, USA
Abstract
While endometriosis typically affects the ovaries, deep
infiltrating endometriosis can affect the gastrointestinal
tract, urinary tract, and deep pelvis, awareness of which
is important for radiologists. Symptoms are nonspecific
and can range from chronic abdominal and deep pelvic
pain to nausea, vomiting, diarrhea, constipation, hema-
turia, and rectal bleeding. Ultrasound and computed
tomography may show nonspecific soft-tissue density
masses causing bowel obstruction and hydronephrosis.
This constellation of presenting symptoms and imaging
evidence is easily mistaken for other pathologies includ-
ing infectious gastroenteritis, diverticulitis, appendicitis,
and malignancy, which may lead to unnecessary surgery
or mismanagement. With this, deep pelvic endometriosis
should be considered in the differential diagnosis in a
female patient of reproductive age who presents with
such atypical symptoms, and further work up with
magnetic resonance imaging is imperative for accurate
diagnosis, treatment selection, and preoperative plan-
ning.
Key words: Endometriosis—Deep infiltrating
endometriosis—Gastrointestinal tract—Pelvis—Cul-de-
sac—Ultrasound—Magnetic resonance imaging
(MRI)—Computed tomography (CT)
Endometriosis was first reported by Rokitansky in 1860
and affects 1–7%of women, including 6–10%of pre-
menopausal women and 2.5%of postmenopausal women
[1–3] with an average age of diagnosis usually between
25- and 29-year old, increasing with age. Risk factors
include prolonged use of an intrauterine device, unin-
terrupted menstrual cycles, and a history of a first-degree
relative with endometriosis [4]. The incidence of
endometriosis increases to 17%in women with infertility
and to 50%of women who complain of pelvic pain [5,6].
Typically, endometriosis implants in the ovaries and
uterosacral ligaments with the classic clinical presenta-
tion being a female of reproductive age with cyclical
pelvic pain with menstruation and dyspareunia [7].
Endometriosis, however, can affect other areas including
the pericardium, lungs, and the peritoneum. Roughly
5–15%of endometriosis affects the gastrointestinal tract
[5,8]. Most commonly, gastrointestinal endometriosis
involves the rectosigmoid colon, followed by the sigmoid
colon, rectum, ileum, appendix, and cecum; this is often
but not always present in conjunction with pelvic
endometriosis.
Deep infiltrating endometriosis (DIE) is defined as
subperitoneal endometrial implants, greater than 5 mm
in depth affecting the gastrointestinal tract, urinary tract,
and pelvic cul-de-sac and is usually associated with
reactive inflammation, fibrosis, adhesions, and smooth
muscle hyperplasia (Fig. 1). Gastrointestinal DIE typi-
cally involves the rectosigmoid, small bowel, colon, and
appendix. DIE of the urinary tract can affect the ureters
and urinary bladder while DIE of the cul-de-sac can in-
volve the uterosacral ligaments, vagina, and cervix. Pa-
tients with endometriosis usually present with chronic,
nonspecific symptoms including nausea, vomiting, diar-
rhea, constipation, rectal bleeding, dyschezia, deep dys-
Correspondence to: Ayeh Darvishzadeh; email: [email protected]
ª
Springer Science+Business Media New York 2016
Abdominal
Radiology
Abdom Radiol (2016)
DOI: 10.1007/s00261-016-0956-8

pareunia, and even crippling, chronic pelvic pain [9,10].
Roughly 27%of intestinal endometriosis results in bowel
obstruction and can necessitate emergency surgery [11,
12].
Since symptoms tend to be nonspecific, the estimated
delay in diagnosis is between 3 and 9 years and is greater
in patients whose primary complaint is pelvic pain as
opposed to those reporting infertility [12,13]. Further-
more, physical exam is usually insensitive to detect
endometriosis [14] with highly variable findings on exam
depending on size and location of ectopic tissue and
clinical experience of examiners. The most common
clinical findings include palpable nodules at the uter-
osacral ligament, rectovaginal space, Pouch of Douglas,
rectosigmoid, and posterior wall of the urinary bladder
[15]. However, the diagnostic value of a physical exam-
ination is limited by the inability of an examiner to
palpate deep enough into the pelvis, specifically in the
rectosigmoid space. Subsequent delayed diagnosis is
costly, with an estimated cost of $12,419 per woman per
year due to health care costs and loss of productivity [16,
17]. Delay in diagnosis leads to more progressive disease,
which increases the risk of organ damage and greater
need for invasive surgical intervention [15].
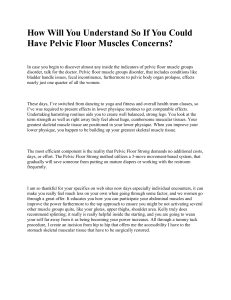
Fig. 1. Schematic of the female reproductive system and
pelvis illustrating typical locations of deep infiltrating
endometriosis. AUterus and associated structures and colon.
BSagittal view of the pelvis.
Fig. 2. Colonoscopy images of female with endometriosis of
the colon showing Amucosal induration with areas of fibrosis
and punctate hemorrhagic foci and Bmass-like protrusion
into the colon.
A. Darvishzadeh et al.: Deep pelvic endometriosis

Fig. 3. An asymptomatic 44-year-old woman with a signifi-
cant family history of colon cancer who on screening colono-
scopy was found to have a mass in the sigmoid colon that did
not penetrate through the mucosa. Differential diagnosis at time
of surgery was gastrointestinal stromal tumor, leiomyoma, or
endometriosis. A,BCoronal and axial contrast-enhanced CT
images show a subtle, soft-tissue density thickening in the
sigmoid colon (arrows). Inlet image is zoomed in image of
coronal CT showing circumscribed mass in colon with hyper-
attenuation at mass borders and heterogenous soft-tissue
density body. CSpecimen of resected sigmoid colon showing
intramural mass protruding into the sigmoid. D–FPathology
images of mass shown in C.DLow-power image of histological,
showing colonic mucosa (arrow) with areas of hypertrophic
muscularis propria and endometriosis (asterisk). EHigh-power
images of benign endometrial gland and endometrial stroma.
FHigh-power image of endometrial gland and stroma stained
positive with estrogen-receptor immunostaining (brown).
A. Darvishzadeh et al.: Deep pelvic endometriosis

Typically, patients with endometriosis are often
diagnosed with pelvic inflammatory disease, irrita-
ble bowel syndrome, Crohn disease, infectious colitis,
diverticulitis, appendicitis, and malignancy [13].
Small, scattered deep endometrial foci can be
especially difficult to detect with computed tomography
(CT) and magnetic resonance imaging (MRI) sec-
ondary to limiting in spatial resolution. Recent devel-
opments in soft-tissue characterization on MRI,
however, allow for excellent preoperative assessment of
DIE. Laparoscopic surgery with histological confirma-
tion remains the gold standard diagnostic method to
date. However, unanticipated intraoperative biopsies
showing endometriosis often result in a second surgery
after reassessment and proper bowel preparation [18].
Given this, diagnosis of endometriosis involving the
colon and pelvis is important to allow for preoperative
planning, which may include a general surgeon or
urologist.
The objective of this article is to review and discuss
the symptoms and imaging of deep pelvic endometriosis
of the gastrointestinal and urinary tract in order to
Fig. 4. 40-year-old female with rectal pain and hematuria. A,
BTransvaginal ultrasound imaging showing a hypoechoic
mass between the urinary bladder and anterior uterus rectum.
C,DAxial and sagittal contrast-enhanced CT images showing
a mildly enhancing mass in between the urinary bladder and
anterior uterus (asterik).
A. Darvishzadeh et al.: Deep pelvic endometriosis

familiarize clinicians with the typical and atypical appear-
ance of suspected DIE on various imaging modalities.
Clinical features and pathophysiology
Deep infiltrating endometriosis consists of subperitoneal
endometrial implants that are greater than 5 mm in
depth. Understanding the imaging of deep infiltrating
endometriosis relies on some factors of its pathophysi-
ology. DIE is associated with reactive inflammation of
the surrounding area, including proliferation of smooth
muscle cells, fibrosis, and adhesions [19]. Endometriotic
implants may also include small, interspersed hemor-
rhagic foci.
Fig. 5. 41-year-old female presented to the Emergency
Department with severe deep pelvic pain. A–CAxial CT
images with enteral contrast showed a lobulated soft-tissue
density mass causing extrinsic compression and severe
luminal narrowing at the rectosigmoid junction. Imaging find-
ings on CT raised concern for a colorectal neoplasm. DSin-
gle-contrast barium enema shows a 7 cm stricture with
serrated appearance and mucosal crenation at the rectosig-
moid junction. Subsequent pathology revealed rectosigmoid
endometriosis.
A. Darvishzadeh et al.: Deep pelvic endometriosis
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
1
/
21
100%