Low Grade Salivary Duct Carcinoma: A Clinicopathologic Study
Telechargé par
Zeggane Abdennour

958
Low
Grade Salivary
Duct
Carcinoma
A
Distinctive Variant with a Low Grade Histology and a Predominant Intraductal
Growth
Pattern
Ruby
Delgado,
M.D.’
David
Klimstra,
M.D.’
Jorge Albores-Saavedra,
M.D.’
Division of Anatomic Pathology, Department
of
Pathology. University of Texas Southwestern
Medical Center, Dallas, Texas.
*
Department
of
Pathology, Memorial Sloan-
Kettering Cancer Center, New
York,
New
York.
The authors thank
Mrs.
R.
Nelly Murillo for her
assistance in the preparation
of
this manuscript.
Address for reprints: Ruby Delgado,
M.D.,
De-
partment
of
Pathology, University
of Texas
Southwestern Medical Ctr., 5323 Harry Hines
Blvd., Dallas.
TX
75235-9072.
Received February 16,
1996;
revision received
May 23, 1996; accepted June 3, 1996.
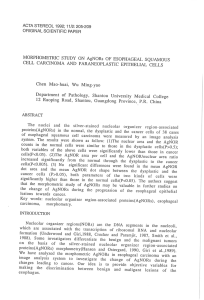
BACKGROUND.
Salivary duct carcinoma
(SDC)
has been established as a morpho-
logically distinct and highly aggressive
(HG)
malignancy of the major salivary
glands. However, a low grade
(LG)
or
intermediate grade salivary duct neoplasm
has not been described.
METHODS.
We report the clinicopathologic findings of
10
cases believed to repre-
sent the
(1.G)
counterpart
of SDC.
lrnmunoperoxidase stains were performed on
tive cases, and electron microscopy
oil
three.
RESULTS.
hll
of the tumors occurred in adult patients with no
sex
predilection,
and presented as slow growing parotid gland lesions.
Four
cases involved the
superficial lobe, one the deep lobe, and
one
arose within an intraparotid lymph
node. The exact location of the tumor within the parotid gland was not stated in
four cases. The size
of
the tumors ranged from
0.7
to
4
cm in greatest dimension,
with most measuring between
1
and
2
cni.
1
he gross appearance was focally to
predominantly cystic. Microscopically, the tumors were characterized by intraduc-
tal proliferative lesions exhibiting three main patterns:
(1)
cystic ducts with micro-
papillaq, tufted, and plaque-like intralurninal projections;
(2)
ducts distended by
a solid
or
pseudocribriform (fenestrated) cellular proliferation,
with
varied cystic
dilatation; and
(3)
ducts exhibiting architectural atypia. The three patterns coex-
isted arid merged in most tumors, in varying proportions.
All
tumors shared bland
to
LG
cytologic features, with the exception
of
one that had focal high-grade cyto-
logic ductal atypia. Despite
gross
circumscription, there was microscopic multifo-
cality, and in one case, stromal invasion.
By
immunohistochemistry the neoplastic
cells expressed the conventional ductal and glandular epithelial cell markers in
addition to strong positivity
for
S-100
with coexpression for
CK-903.
Electron mi-
croscopy
contirmrd
the ductal phenotype
of
the tumors and supported
an
in situ
process evidenced by the presence
of
native myoepitlielial cells. Nine patients
underwent total parotidectoniy and one superficial parotidectorny. One patient
received radiation therapy following total parotidecotmy. Follow-up for
6
cases
ranged from
2
to
12
years and revealed no evidence of disease.
CONCLUSIONS.
LG-SDC represents the
LG
end of the spectrum
of
salivary duct
malignant neoplasms anti exhibits differentiation towards an intercalated duct-
like cell phenotype. Its relationship
to
1IG-SL)C
should be Purther explored.
Cancer
1996; 78:958-67.
0
I996
American Curicer Society.
KEYWORDS
salivary gland, duct carcinoma,
low
grade, high grade, immunohisto-
chemistry, electron microscopy.
lthough the histomorphogenesis
of
some salivary gland neo-
A
plasms remains unclarified, the
term
salivary duct carcinoma
(SDC)
has
been restricted to tumors composed predominantly
or
ex-
clusively of ductal cells with the formation of structures resembling
distended salivary ducts. In most instances
SDC
has been recognized
by
its striking resemblance to mammary duct carcinoma. To date
c)
1996 American Cancer Society

Low
Grade Salivary Duct Carcinoma/Delgado et al.
959
TABLE
I
Immunohistouhemical Findings in Five Cases
of
LG-SDC
No.
of
immunoreactive
Antibody
CaSeS
Pattern
of
immunoreactivity
S-100
protein
3
SM!\
1
membranous
>
cytoplasmic
diffusea;
i
menibrdnous
>
cpoplasniic
diffusea:
4
t14+*
luniinal diffuse;
7
-
c
cpplasmic focahpocrine
metaplastic
cells;
A
+
nuclear
&
ryoplasmic diffiise"'';
cytoplasmic limited
to
T-4
myoepithelial cells;
-4
+
I.G-SI)C:
lowgradi
salig
dutr
carcinoma;
pCE4:
polyclonal carcinoenibryonic
anrign;
CCIEP
gross
c!\rir
diww lluij
prorein;
!N\:
smoorh
muscle
spPrific aciin
Inrludrr
yacuol;i[rd
c~lls.
liitl:itle(i
some
of
[he
nyqi~helial
(ells.
Snurtv
&
I)iluunrl:
(:\iokeraun
Cnm
5.2
(Hecron-[)ickinson.
\,luun[ain
View.
CAiPrediluredi:
Cvokera-
iiii
\lA(IOJ
;Em
lhgnoslicr
Inc.
Srw
York,
NI':I:?Ol:
pCE4
il)ako
Corporalion.
Carpinierta.
CNI:40;;
HEY-?
hignrt
:
abiiralorie,
Inc,
Dcdhani.
S1hil:IOOi;
S-I00
prolein
:Dako
Corporaiion,
Carpinreria,
C4i1.300!,
5\19
6ignia
Ihgnosrics,
Sr.
1.ouir.
MOil:100i.
only a high grade SIX has been recognized, showing
the characteristic in situ and invasive growth phases.'."
During our review of SDCs we encountered tu-
mors characterized by the proliferation of salivary duct
structures and exhibiting ductal differentiation (by
light microscopy, immunohistochemistry, and elec-
tron microscopy), but lacking both the aggressive mor-
phologic features and clinical behavior of the high
grade
SIX
We
believe these tumors represent the low
grade end of the spectrum of salivary duct malignan-
cies.
MATERIALS AND METHODS
Four cases were accrued in consultation.
A
fifth case
was retrieved from the surgical pathology files of Park-
land Memorial Hospital in Dallas, Texas, and the re-
maining five from the surgical patholoby files of Me-
morial Hospital in New York, New York. Clinical infor-
mation and follow-up data were provided by the
referring physicians in three cases and from the pa-
tients' charts in four cases; three patients were lost
to follow-up. Routine hematoxylin and eosin stained
sections were examined. Additional sections from all
cases were prepared for histochemical, periodic acid-
Schiff (PAS), and mucicarmine, and immunohisto-
chemical analysis. Immunostains were performed us-
ing the standard avidin-biotin peroxidase method.
Commercially available antibodies were used with ap-
propriate controls (Table
1).
In one case fresh tissue was fixed in glutaralde-
hyde and routinely processed for transmission elec-
tron microscopic examination. Selected tumoral tissue
was retrieved from paraffin embedded blocks in the
other two cases. The tissue was processed following
deparaffinization in xylene and rehydration through
graded ethanol solutions.
All
tumors were examined
in a
JEOL
1200
electron microscope
(JEOL
Ltd., Tokyo,
Japan).
CLINICAL FINDINGS
A
clinical summary of all cases is provided in Table
2.
PATHOLOGIC FINDINGS
Microscopically, the tumors were characterized by a
heterogeneous intraductal proliferative process with
three dominant patterns
or
components:
(1)
cystically
dilated ducts exhibiting partial to circumferential in-
tracystic micropapillary and tufted formations focally
anastomosing and coalescing into solid plaque-like
epithelial stratification (Figs. IA-C). The micropapil-
lae were composed of cuboidal to small columnar cells
exhibiting conspicuous intracytoplasmic microvacu-
oles which increased in number from base
to
lumen
and were accompanied by a fine granular yellow-
brown pigment. In its fullest expression the cells were
filled and distended by sharply outlined minute vacu-
oles causing indentation of the nucleus and accentua-
tion of the cytoplasmic rim, resulting in scallop-
shaped micropapillae (Figs.
2A,
B). Better developed
papillae with fibrotic fibrovascular cores and psam-
moma bodies were also present. In the nonprolifera-
tive areas the cysts were lined by a simple apocrine
epithelium showing attenuation and squamous meta-
plasia.
(2)
Ducts distended by solid, pseudocribriform
(fenestrated) or solid-papillary ductal proliferation
(Fig.
3A).
The cells comprising these neoplastic ducts
were ovoid to cuboidal with dense pale to bright eosin-
ophilic cytoplasm, indistinct cell borders, and oval nu-
clei with finely dispersed chromatin and pinpoint
nucleoli. Foci of apocrine metaplasia were also seen
(Fig.
313,
inset). The cells were arranged in a somewhat
loose to overlapping fashion forming solid sheets
or
slit-like to irregular luminal spaces
or
fenestrae re-
sulting in a pseudocribriform appearance (Fig.
38).
The spaces contained basophilic mucin alternating
with hyaline colloid-like material. Many of the ducts
showed cystic dilatation in varying degrees and were
filled by basophilic mucin. This cystic change was ac-
companied occasionally by the intracytoplasmic mi-
crovacuolar change previously described. Other ducts
had a solid-papillary appearance consisting of solid
sheets traversed by delicate fibrovascular cores.
(3)
Ducts displaying conventional architectural atypia,
spanning the entire range of mild to severe (Fig.
4).
All

960
CANCER September
1,1996
I
Volume
78
I
Number
5
TABLE
2
Clinicopathologic Findings
in
Ten Patients with
Low
Grade Salivary Duct Carcinoma
Case
#
Age
(yrs)/sex
Location Size Original
diagnosis
Treatment
Follow-up
1
58iM
Parotid [superficial
lobe;
I
cni Lowgrade papillocystic adeiiocarriiioma Superficial parotidectomy
-
62iF
Parotid
0.7
rni
Papillocystic carcinoma Parotidectomy
-
?
3
32iF
Right parotid (superfiria!
lobe)
1.1
ciii
Acinic
cell
carcinoma; positive margins Parotidectomy, radiotherapy NED at
12
yrs
4
63\11!
Right parotid (superficial
lobel
1.3
ciii
Aciiiic
cell
carcinoma Parotidectomy
NED
at
I1
yrs
6
56iF Right parotid
I
cni Acinic
cell
carcinoma Parotidectomy NED
at
2
yrs
n
69iF
Right parotid (intraparotid lymph
node1
4
cni
LG-SDC Parotidectomy
NED
a1
2
)rs
9
69
/
M
I.eR
parotid
0.9
cm
LG-SDC Parotidectomy
in
52iF
Right parotid (deep
lobe)
0.8
cm
LG-SDC with
focal
invasion; positive margins Parotidectomy, radiotherapy
NED
at
9
mos
NED:
no
evidence
of
disease;
LG-SDC:
low
gade salivary duct carcinoma,
J
i4iM
Left
parotid
1.8
ciii
Aciiiic ceil carcinoma Parotidectomy NED at
6
17s
I
4?/M
Left parorid (superficial
lobe)
1.2
ciii
LG-SDC
Parotideclomy NED at
2
ITS
FIGURE
1.
Papillocystic pattern
of
low
grade salivary duct carcinoma. (A)
Delicate filigreed intracystic micropapillae
with
psamrnoma body rnicrocalcifi-
cation (arrow).
(8)
Anastornosing micropapillae.
(C)
Mural tufting.
three patterns coexisted and merged in most tumors
in varying proportions and combinations. (The first
pattern was observed in
100%
of
the cases, the second
in
90%,
and the third in
60%).
In the cases where a
large cyst dominated the histologic picture, the other
two components were found in
a
pericystic arrange-
ment and focally communicating with the major cyst.
All tumors were nonencapsulated but somewhat cir-
cumscribed by a dense sclerotic stroma exhibiting sec-
ondary changes such
as
remote hemorrhage, choles-

Low
Grade Salivary Duct CarcinomalDelgado et al.
961
FIGURE
2.
Intracytoplasrnic vacuolar change in papillocystic
low
grade salivary duct carcinoma.
(A)
Transition from apocrine-like cells
to
vacuolated
cells,
with
progressive accumulation of intracytoplasmic microvacuoles.
(B)
Vacuolated ductal cells are filled and distended by nonmernbrane bound
lipid droplets, anG show surface microvilli.
terol granulomas, and dystrophic calcification. Also
bordering the tumors was a marked lymphoid infil-
trate (Fig.
I,
bottom).
Despite the apparent circumscription of the tu-
mors, detached tumor foci were seen in the sur-
rounding glandular parenchyma (Fig.
5),
best interpre-
ted as niultifocality, and in one case, stromal microin-
vasion (Fig.
CiB)
was noted disclosing its malignant
potent ial.
Onc
tumor was remarkable for having originated
in an intraparotid lymph node, extending beyond it
into the immediate parotid parenchyma and sur-
rounding but
not
invading peripheral nerve branches.
Mitotic activity was negligible in
most
cases, non-
atypical mitotic figures being identified in two cases.
Mucicarrnine and PAS stains highlighted the ma-
tctrial in intercellular spaces, with no intracytoplasmic
niiicin positivity observed.
No
PAS-positive diastase
resistant material suggestive
of
zymogen granules
could be identified. Large PAS-diastase positive gran-
ules were present but confined to foci of apocrine
m
e
t
a
pl asia.
Immunoperoxidase studies revealed the expected
reactivity to conventional epithelial markers (Table
1).
Of significance, however, was the strong nuclear and
cytoplasmic positivity for
S-100
protein (Fig.
7)
and the
cytoplasmic positivity for the high molecular weight
cytokeratin
(3413E12
or
MA903).
All
three morphologic
components exhibited similar immunostaining pat-
terns, and encompassed the vacuolated and nonvacu-
olated cells. In addition, smooth muscle actin outlined
the ductal proliferative lesions in a pattern indicative
of
a
myoepithelial layer of pre-existing ducts involved
by an intraductal neoplastic proliferation (Fig.
8A).
Similarly, collagen type
IV
antibodies circled the neo-
plastic ducts. Immunoreactivity
for
antibodies to
GCDFP-15,
observed in two cases, correlated with foci
of apocrine metaplasia.
Ultrastructurally, the tumors were composed
of
ductal cells with interdigitating cell membranes form-
ing intercellular lumina and bound by a continuous
basal lamina. The ductal cells displayed apical micro-
villi and contained a modest number of organelles,
except for occasional cells showing an increased num-
ber of mitochondria.
Also
identified
in
a peripheral
or
basal location were myoepithelial cells with long
attenuated cytoplasmic prolongations (Fig.
8B).
The
vacuolated cells were characterized as plump ductal
cells distended by what appeared as coalescing empty
nonmembrane bound spaces in some cells and lipid
droplets in others. These caused significant indenta-
tion of the nuclei and displaced the cytoplasmic organ-
elles to a subplasmalemmal location (Fig.
2R).
DISCUSSION
We report ten cases
of
a tumor which conforms to the
cytoarchitectural definition
of
a salivary duct neo-
plasm (composed primarily of ductal luminal cells
with formation of distended salivary duct structures),
that, to
our
knowledge, has not been previously char-
acterized as such. Because
it
exhibits a bland histo-
morphology and has thus far demonstrated a favorable
behavior, we propose the term “low grade salivary
duct carcinoma”
(IG-SDC).

962
CANCER
September 1,1996
/
Volume
78
/
Number
5
FIGURE
3.
(A)
Classic pseudocribriform pattern
of
low
grade salivary duct carcinoma
(B)
Proliferating ductal cells
show
somewhat overlapping
oval nuclei and indistinct cytoplasmic cell borders. Irregular intercellular spaces are filled with hyaline material. Focus of apocrine rnetaplasia (inset).
In contrast to its aggressive counterpart, the high
HG-SDC,’-6
salivary duct neoplastic proliferations
grade salivary duct carcinoma
(HG-SDC),
better have demonstrated a more aggressive behavior than
known for its reiterated similarity to breast duct carci- their morphologic counterparts in the breast. This ap-
noma (mainly comedo type),’-6
LG-SDC
spans an ap- parent organ-specificity may
be
related to underlying
pearance reminiscent of florid to atypical ductal hy- structural differences
(i.e.,
regional anatomy or glan-
perplasia to
low
grade intraductal breast carcinoma dular microanatomy), to biologic differences (i.e., hor-
(Table
3).
Based on the accumulated experience with monal regulation), andlor to inherent tumor proper-
 6
7
8
9
10
6
7
8
9
10
1
/
10
100%