LOCAL ANAESTHETICS
Dr. Sanjita Das

•Local anesthetics are the agents which on topical application or local injection cause
reversible loss of sensory perception, especially pain in a localized area of the body.
•Local anesthesia is any technique to render part of the body insensitive to pain without
affecting consciousness.
•These cause loss of sensory as well as motor impulses.
•No local damage to the neurons.
•In many situations, such as cesarean section, it is safer and therefore superior to general
anesthesia.
•It is also used for relief of non-surgical pain and to enable diagnosis of the cause of some
chronic pain conditions.
•Anesthetists sometimes combine both general and local anesthesia techniques.

Techniques
•Surface anesthesia - application of local anesthetic spray, solution or cream to
the skin or a mucous membrane. The effect is short lasting and is limited to the
area of contact.
•Infiltration anesthesia - injection of local anesthetic into the tissue to be
anesthetized. Surface and infiltration anesthesia are collectively topical
anesthesia.
•Field block -subcutaneous injection of a local anesthetic in an area bordering
on the field to be anesthetized.
•Peripheral nerve block - injection of local anesthetic in the vicinity of a
peripheral nerve to anesthetize that nerve's area of innervation.
•Plexus anesthesia - injection of local anesthetic in the vicinity of a nerve
plexus, often inside a tissue compartment that limits the diffusion of the drug
away from the intended site of action. The anesthetic effect extends to the
innervation areas of several or all nerves stemming from the plexus.
•Epidural anesthesia - a local anesthetic is injected into the epidural space
where it acts primarily on the spinal nerve roots. Depending on the site of
injection and the volume injected, the anesthetized area varies from limited
areas of the abdomen or chest to large regions of the body.
•Spinal anesthesia - a local anesthetic is injected into the cerebrospinal fluid,
usually at the lumbar spine (in the lower back), where it acts on spinal nerve
roots and part of the spinal cord. The resulting anesthesia usually extends from
the legs to the abdomen or chest.
•Intravenous regional anesthesia (Bier's block)- blood circulation of a limb is
interrupted using a tourniquet (a device similar to a blood pressure cuff), then a
large volume of local anesthetic is injected into a peripheral vein. \
•Local anesthesia of body cavities (e.g. intrapleural anesthesia, intraarticular
anesthesia)

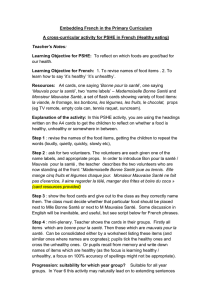
LAs bind and inhibit many differing
receptors and channels
•Channels
–Na
–Ca (multiple types)
–K
•Enzymes
–Adenylyl cyclase
–Guanylyl cyclase
–Lipases
•Receptors
–Nicotinic
acetylcholine
–NMDA
–β2-adrenergic
•Important for
spinal, epidural, or
systemic effects?
Anesthesiology 1990; 72:711-34

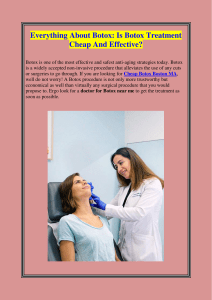
Mechanism of action
•The mechanism of local anesthetics
connects with the ion channels, nerve,
and depolarization.
•Block the conduction in peripheral
nerves that inhibited the nerve to
excited and created anesthesia.
•The anesthetic is a reversible reaction.
It binds and activates the sodium
channels.
•The sodium influx through these
channels and depolarizes the nerve cell
membranes. It also created high
impulses along the way.
•As a result, the nerve loses
depolarization and the capacity to
create the impulse, the patient loses
sensation in the area supplied by the
nerve.
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
1
/
67
100%