Spectrochimica
Acta
Part
A
92 (2012) 318–
324
Contents
lists
available
at
SciVerse
ScienceDirect
Spectrochimica
Acta
Part
A:
Molecular
and
Biomolecular
Spectroscopy
j
our
na
l
ho
me
p
age:
www.elsevier.com/locate/saa
Quantification
of
creatinine
in
biological
samples
based
on
the
pseudoenzyme
activity
of
copper–creatinine
complex
Padmarajaiah
Nagaraja∗,
Krishnegowda
Avinash,
Anantharaman
Shivakumar,
Honnur
Krishna
Department
of
Studies
in
Chemistry,
University
of
Mysore,
Manasagangothri,
Mysore
570006,
India
a
r
t
i
c
l
e
i
n
f
o
Article
history:
Received
20
November
2011
Received
in
revised
form
19
February
2012
Accepted
23
February
2012
Keywords:
Creatinine
Serum
Urine
Jaffe’s
Pseudoenzyme
a
b
s
t
r
a
c
t
Glomerular
filtration
rate
(GFR),
the
marker
of
chronic
kidney
disease
can
be
analyzed
by
the
concentra-
tion
of
cystatin
C
or
creatinine
and
its
clearance
in
human
urine
and
serum
samples.
The
determination
of
cystatin
C
alone
as
an
indicator
of
GFR
does
not
provide
high
accuracy,
and
is
more
expensive,
thus
measurement
of
creatinine
has
an
important
role
in
estimating
GFR.
We
have
made
an
attempt
to
quantify
creatinine
based
on
its
pseudoenzyme
activity
of
creatinine
in
the
presence
of
copper.
Crea-
tinine
in
the
presence
of
copper
oxidizes
paraphenylenediamine
dihydrochloride
(PPDD)
which
couples
with
dimethylamino
benzoicacid
(DMAB)
giving
green
colored
chromogenic
product
with
maximum
absorbance
at
710
nm.
Kinetic
parameters
relating
this
reaction
were
evaluated.
Analytical
curves
of
creatinine
by
fixed
time
and
rate
methods
were
linear
at
8.8–530
mol
L−1and
0.221–2.65
mmol
L−1,
respectively.
Recovery
of
creatinine
varied
from
97.8
to
107.8%.
Limit
of
detection
and
limit
of
quan-
tification
were
2.55
and
8.52
mol
L−1respectively
whereas
Sandell’s
sensitivity
and
molar
absorption
coefficient
values
were
0.0407
g
cm−2and
0.1427
×
104L
mol−1cm−1respectively.
Precision
studies
showed
that
within
day
imprecision
was
0.745–1.26%
and
day-to-day
imprecision
was
1.55–3.65%.
The
proposed
method
was
applied
to
human
urine
and
serum
samples
and
results
were
validated
in
accor-
dance
with
modified
Jaffe’s
procedure.
Wide
linearity
ranges
with
good
recovery,
less
tolerance
from
excipients
and
application
of
the
method
to
serum
and
urine
samples
are
the
claims
which
ascertain
much
advantage
to
this
method.
© 2012 Published by Elsevier B.V.
1.
Introduction
Estimation
of
glomerular
filtration
rate
(GFR)
is
the
most
widely
used
test
for
assessing
renal
function
[1].
Functions,
which
mea-
sure
the
GFR
directly
or
indirectly,
are
major
tools
to
assess
the
extent
of
impairment
of
renal
function.
The
most
exact
technique
for
measuring
the
GFR
requires
the
infusion
of
radioisotopes
such
as
51chromium-EDTA, 125I-iothalamate, 99mTc-DTPA
or
radio
contrast
agents
such
as
iohexol,
or
inulin
[2],
which
do
not
get
reabsorbed,
secreted
or
metabolized
by
the
kidney.
These
methods
require
intravenous
and
timed
collection
of
multiple
plasma
and
urine
samples
making
the
analytical
methods
highly
cumbersome
and
difficult
to
apply
in
routine.
Abbreviations:
PPDD,
paraphenylenediamine
dihydrochloride;
DMAB,
dimethy-
lamino
benzoicacid;
QCM,
quality
control
material;
KP,
Michaelis–Menten
constants
for
PPDD;
KD,
Michaelis–Menten
constant
for
DMAB;
KC,
Michaelis–Menten
con-
stants
for
copper;
KCr,
Michaelis–Menten
constants
for
creatinine;
Vmax,
maximum
rate
of
the
reaction
at
optimized
reagent
concentration.
∗Corresponding
author.
Tel.:
+91
821
2412557;
fax:
+91
821
2421263.
E-mail
addresses:
(P.
Nagaraja).
Another
method
for
the
estimation
of
GFR
is
urinary
measure-
ment
of
cystatin
C
[3]
an
endogenous
protein
belonging
to
the
type
2
cystatin
gene
family.
Reports
have
shown
that
cystatin
C
levels
get
altered
in
patients
with
cancer
[4],
thyroid
dysfunction
[5].
Cystatin
C
levels
are
also
affected
by
cigarette
smoking
and
by
C-reactive
proteins
[6],
which
might
or
might
not
reflect
actual
renal
dysfunc-
tion
[7].
The
role
of
cystatin
C
to
monitor
GFR
during
pregnancy
remains
controversial
[8].
The
use
of
cystatin
C
alone
as
a
determi-
nator
of
GFR
does
not
yield
high
accuracy
over
isotope
dilution
mass
spectrometry-based
Modification
of
Diet
in
Renal
Disease,
and
it
is
also
more
expensive
[9].
Measurement
of
creatinine
content
and
its
clearance
in
urine
and
serum
samples
is
the
legend
for
the
GFR
estimation.
Although,
multi-shot
technique
is
more
convenient,
but
measurement
of
creatinine
and
its
clearance
are
still
the
methods
of
choice
most
commonly
followed
for
assessing
the
renal,
muscular,
cardiac
[10],
and
thyroid
functions
[11].
Jaffe’s
alkaline
sodium
picrate
method
is
the
most
widely
accepted
standard
method
for
creatinine
measurement
[12].
But
this
method
is
affected
by
many
chemical
species
such
as
creatine,
bilirubin,
hemoglobin,
cefoxitin
and
cephalothin
[13].
Numerous
modifications
to
Jaffe’s
reaction
have
been
effected
to
elimi-
nate
or
reduce
interferences,
which
include
specific
adsorption
of
1386-1425/$
–
see
front
matter ©
2012 Published by Elsevier B.V.
doi:10.1016/j.saa.2012.02.104

P.
Nagaraja
et
al.
/
Spectrochimica
Acta
Part
A
92 (2012) 318–
324 319
creatinine,
removal
of
interfering
compounds,
dialysis,
adjusting
the
pH,
and
kinetic
measurements.
Unfortunately,
none
of
these
modifications
were
capable
of
completely
eliminating
interfer-
ences.
Spectrophotometric
method
based
on
multi-enzyme
system
has
been
developed
to
improve
the
specificity
of
creatinine
deter-
mination
[14].
The
method
gives
accurate
result
but
is
of
much
imprecise
and
also
expensive.
Moreover,
the
use
of
multi-enzyme
system
requires
caution,
because
of
the
increase
in
the
risk
of
interference
with
increases
in
the
number
of
the
enzymes
used
[15].
Other
spectrophotometric
methods
for
the
assay
of
cre-
atinine
concentration
include
3,5-dinitrobenzoic
acid
[16,17],
3,5-dinitrobenzoyl
chloride
[18,19],
methyl-3,5-dinitrobenzoate
in
a
mixture
of
dimethyl
sulfoxide,
methanol,
and
tetramethyl
ammonium
hydroxide
[20],
1,4-naphthoquinone-2-sulfonate
[21],
Sakaguchi’s
color
reaction
of
creatinine
with
o-nitrobenzaldehyde
[22],
capillary
electrophoresis
[23–25],
liquid
chromatography
(LC)
[26],
gas
chromatography
(GC)
[27],
GC
with
isotope
dilution
mass
spectrometry
[28],
and
tandem
mass
spectrometry
[29,30].
Most
of
these
methods
have
serious
limitations
with
respect
to
their
sensitivity,
linearity,
precision
and
applicability.
In
most
instances,
the
conditions
required
for
best
sensitivity,
stoichiometry
(linear-
ity
or
range),
and
for
the
elimination
of
interferences
have
not
been
delineated
properly.
A
new
spectrophotometric
method
based
on
enzyme
like
activ-
ity
of
copper–creatinine
complex
[31]
was
developed
to
determine
creatinine
in
serum
and
in
urine
samples.
The
performance
of
the
method
was
evaluated
and
potential
interferences
were
studied.
Results
obtained
using
the
proposed
method
was
compared
to
the
ones
achieved
with
a
modified
Jaffe’s
procedure.
2.
Experimental
2.1.
Instrumentations
A
JASCO
model
UVIDEC-610
PC
double
beam
spectrophotome-
ter
with
1
cm
matched
quartz
cells
was
used
for
all
measurements.
Serum
samples
were
centrifuged
using
Remi
R24
(Mumbai,
India)
desktop
centrifuge
having
17,200
rpm
and
27,440
RCF.
A
Remi
cyclomixer
was
used
for
mixing
of
the
reaction
mixture.
pH
of
the
solution
was
measured
using
Chemlabs
(Nairobi,
Kenya)
pH
meter.
Lab
Dispo
sodium
heparin
tubes
containing
18
I.U.
of
sodium
heparin
obtained
from
Manshe
Healthcare,
Ahmed-
abad,
India,
was
used
to
store
the
blood
samples
drawn
from
donors.
2.2.
Reagents
and
solutions
All
chemicals
used
in
the
assay
were
of
analytical
grade.
Solutions
were
freshly
prepared
in
double
distilled
water
and
stored
in
amber
colored
standard
flasks
and
refrigerated
at
−4◦C
until
use.
Paraphenylenediamine
dihydrochloride
(PPDD)
(Merck,
Germany)
(1.656
mmol
L−1)
was
prepared
by
dissolving
3
mg
of
this
reagent
in
water
to
prepare
a
10
mL
solution.
Dimethylamino
benzoicacid
(DMAB)
(Himedia
Ltd.,
India)
(181.18
mmol
L−1)
was
prepared
by
dissolving
300
mg
of
this
reagent
in
0.5
mL
of
0.01
mol
L−1hydrochloric
acid
solution
and
then
adjusting
the
volume
of
solution
to
10
mL
with
water.
A
1.6
mmol
L−1cop-
per
(II)
sulfate
pentahydrate
(Himedia)
solution
was
prepared
by
dissolving
4
mg
of
the
salt
in
water
to
achieve
a10
mL
solution.
Creatinine
was
purchased
from
S.D.
Fine
Laboratory,
Mumbai,
India
and
the
required
standard
solutions
were
prepared
by
dissolving
suitable
amount
of
creatinine
in
double
distilled
water.
2.3.
Biological
samples
Blood
and
urine
samples
were
collected
from
volunteers
follow-
ing
Institutional
Human
Ethical
Committee
guidelines
(IHEC
–
UOM
No
22/Ph.D/2008-09).
The
blood
samples
obtained
from
the
donors
was
centrifuged
and
stored
in
Dispo
sodium
heparin
tubes
at
−4◦C
till
use.
2.4.
Quantification
of
creatinine
by
kinetic
and
fixed
time
method
The
concentration
of
creatinine
was
determined
kinetically
in
3
mL
of
the
solution
containing
55
mol
L−1PPDD,
6
mmol
L−1
DMAB
and
53.3
mol
L−1copper
in
1
mmol
L−1potassium
dihy-
drogen
orthophosphate/sodium
hydroxide
buffer
of
pH
7.8.
The
reaction
was
initiated
at
25 ◦C
by
adding
100
L
of
different
con-
centrations
of
creatinine
within
the
linearity
range.
The
change
in
the
absorbance
was
continuously
recorded
at
710
nm
for
5
min
as
a
function
of
reaction
rate.
The
analytical
curve
for
creatinine
quantification
by
one
time
assay
method
was
obtained
from
a
final
3
mL
volume
of
the
solution
containing
55
mol
L−1PPDD,
6
mmol
L−1DMAB
and
53.3
mol
L−1copper
in
1
mmol
L−1potassium
dihydrogen
ortho
phosphate/sodium
hydroxide
buffer
at
pH
7.8
and
100
L
of
var-
ious
concentrations
of
creatinine
within
the
linearity
range.
The
reaction
mixture
was
allowed
to
stand
for
20
min
at
room
tempera-
ture.
Absorbance
of
the
colored
solution
was
recorded
with
respect
to
blank
containing
all
optimized
reagents
except
creatinine.
2.5.
Evaluation
of
kinetic
constants
Michaelis–Menten
constant
values
were
obtained
as
indicated
in
the
literature
[32,33].
The
initial
velocities
(Vo)
were
determined
as
a
function
of
the
reagents:
creatinine
(Co),
PPDD
(Po),
DMAB
(Do)
and
Cu2+ (Cuo).
Experiments
were
made
in
a
univariate
way
by
varying
the
concentration
of
one
of
the
reagents
at
a
time.
Experi-
ments
were
repeated
using
different
concentrations
of
creatinine.
3.
Results
and
discussion
3.1.
Effect
of
pH
The
following
buffers
with
concentration
range
of
0.1–10
mmol
L−1were
kinetically
studied
for
the
assay
namely,
citric
acid/potassium
citrate
at
pH
3.6–5.6,
acetate/acetic
acid
at
pH
3.6–5.6,
potassium
dihydrogen
phosphate/sodium
hydroxide
at
pH
6.0–8.0,
potassium
dihydrogen
orthophos-
phate/dipotassium
hydrogen
orthophosphate
at
pH
6.0–7.8
and
tris
amine/hydrochloric
acid
buffer
at
pH
7.6–10.
The
maximum
reaction
rate
was
recorded
with
potassium
dihydrogen
phos-
phate/sodium
hydroxide
buffer
at
pH
7.8.
Hence
all
further
studies
were
carried
out
with
potassium
dihydrogen
phosphate/sodium
hydroxide
buffer
which
offered
the
maximum
reaction
rate
in
its
1
mmol
L−1solution.
3.2.
Temperature
sensitivity
Effect
of
temperature
on
the
sensitivity
of
the
assay
was
determined
by
incubating
3
ml
of
reaction
mixture
containing
55
mol
L−1PPDD,
6
mmol
L−1DMAB,
53.3
mol
L−1copper
and
176
mol
L−1of
creatinine
in
1
mmol
L−1potassium
dihydrogen
ortho
phosphate/sodium
hydroxide
buffer
at
pH
7.8
at
different
temperatures
(0–80 ◦C)
for
20
min.
The
result
indicated
that
the
colored
product
formed
was
stable
in
the
temperature
range
of
20–35 ◦C.
Any
further
increase
in
the
temperature
initiated
the
decomposition
process
with
the
corresponding
decrease
in
the
absorbance
values;
decrease
in
temperature
lowered
the
time

320 P.
Nagaraja
et
al.
/
Spectrochimica
Acta
Part
A
92 (2012) 318–
324
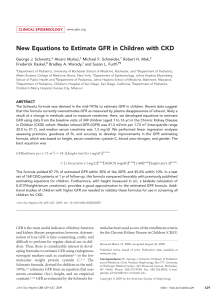
Fig.
1.
Suggested
reaction
mechanism
for
the
formation
of
green
colored
product.
needed
for
completion
of
reaction.
Hence
all
analyses
were
carried
out
at
the
optimum
room
temperature.
3.3.
Proposed
reaction
mechanism
The
probable
reaction
mechanism
involved
for
the
copper–creatinine
catalyzed
reaction
of
PPDD
and
DMAB
is
as
proposed
in
Fig.
1.
Under
optimum
reaction
conditions
when
copper
and
creatinine
are
present,
PPDD
looses
two
electrons
and
two
protons
forming
electrophillic
1,4-diimine,
which
may
act
as
the
oxidative
coupling
species.
The
1,4-diimine
undergoes
electrophillic
substitution
with
DMAB
in
the
free
para
position
to
the
N,N-dimethylamino
group,
forming
green-colored
product
having
strong
absorption
at
710
nm
Fig.
2.
Analytical
curve
for
the
quantification
of
creatinine
by
the
rate
method.

P.
Nagaraja
et
al.
/
Spectrochimica
Acta
Part
A
92 (2012) 318–
324 321
Table
1
Within
day
and
day
to
day
imprecisions.
Within
day
imprecisionaDay
to
day
imprecisiona
X
(mol
L−1)
SD
CV
n
X
(mol
L−1)
SD
CV
n
88
0.0018
1.26
10
88
0.0049
3.623
20
265
0.0034
0.82
10
265
0.0085
2.05
20
442
0.0045
0.745
10
442
0.0096
1.553
20
X
=
creatinine;
n
=
number
of
runs.
aDuplicate
measurement.
3.4.
Analytical
parameters
The
initial
reaction
rate
obtained
by
kinetic
method
for
the
quan-
tification
of
creatinine
was
plotted
against
the
concentration
of
creatinine
to
get
the
analytical
curve.
The
values
of
KCr and
Vmax
for
creatinine
from
the
Lineweaver–Burk
plot
were
found
to
be
3.33
mol
L−1and
0.0668
min−1,
respectively.
The
linear
response
range
was
from
0.22
to
2.65
mmol
L−1of
creatinine.
The
analytical
curve
for
quantification
of
creatinine
is
depicted
in
Fig.
2.
The
lin-
ear
regression
equation
of
the
straight
line
as
shown
in
Fig.
2
is
rate
=0.034Ccreatinine +
0.001.
Michaelis–Menten
constants
for
PPDD,
DMAB
and
copper
were
determined
by
double
reciprocal
plot
in
the
concentrations
range
of
13.75–55
mol
L−1,
0.6–6
mmol
L−1and
5.33–53.3
mol
L−1,
respectively.
Creatinine
concentrations
of
0.44,
0.88,
1.76
and
2.65
mmol
L−1in
the
final
volume
of
3
mL
were
used
for
each
kinetic
study.
The
KP,
KDand
KCwere
found
to
be
27.07
mol
L−1,
2.65
mmol
L−1and
222
mol
L−1,
respectively.
Constant
intercept
was
obtained
in
a
double-reciprocal
plot
of
Voversus
Po,
Doand
Cuo
(panels
A–C
of
Fig.
3)
at
different
concentrations
of
creatinine.
The
method
based
on
measurements
made
after
20
min
of
reac-
tion
time
indicated
a
linear
response
(absorbance)
in
function
of
the
concentration
of
creatinine
(Fig.
4)
over
the
range
from
8.8
to
530
mol
L−1.
Analytical
curve
equation
was
=0.0015Ccr +
0.0058
with
a
regression
coefficient
of
0.999.
The
molar
absorption
coef-
ficient
was
0.1427
×
104L
mol−1cm−1and
the
RSD
was
0.00886
(n
=
10).
Sandell’s
sensitivity
was
studied
to
determine
the
concentra-
tion
of
creatinine
required
to
obtain
the
lower
absorbance
of
0.01;
the
study
revealed
that
0.04
g
cm−2of
creatinine
in
the
opti-
mized
reaction
mixture
yields
0.01
absorbance.
Limit
of
detection
and
limit
of
quantification
were
2.55
mol
L−1and
8.52
mol
L−1
respectively.
Recovery
studies
were
conducted
in
human
urine
and
serum
samples
by
spiking
standard
creatinine
to
the
calculated
diluted
samples.
The
magnitude
of
total
imprecision
of
the
proposed
method
was
studied
by
analyzing
reaction
mixture
containing
known
concen-
trations
of
creatinine
within
Beer’s
law
range;
three
concentrations
Table
2
Interference
study
by
excipients.
Interferants
Tolerance
ratioa
EDTAb0.1
Iron
II,
iron
III,
bilirubin,
nitrite 0.6
Nickel,
phosphate,
ascorbic
acid,
citrateb4
Aminophylline,
heparinbhemoglobin
8
Gentamycin,
diazepam,
amoxycillin
11
Magnesium,
aluminum,
nitrate,
ammonium
14
Uric
acid
24
Glycine,
potassium,
sodium
35
Lactose,
sucrose
50
Carbonate,
bicarbonate,
calcium
75
Glucose,
acetone
90
Urea
95
Creatine,
chloride 150
aTolerance
ratio
corresponds
to
the
ratio
of
limit
of
inhibiting
species
concentra-
tion
to
that
of
152
mol
L−1creatinine
used.
bAnti
coagulants.
Fig.
3.
Kinetic
behavior
of
PPDD
and
DMAB
with
respect
to
various
concentration
of
creatinine.
of
creatinine
ranging
from
lower
to
higher
concentrations
were
selected
with
10
runs
in
a
day
with
a
time
gap
of
1
h
for
within
day
assay
and
20
runs
with
a
time
gap
of
1
day
for
day
to
day
assay.
Results
are
shown
in
Table
1.
Results
showed
that
within
day
impre-
cision
were
0.745–1.26%
(n
=
10)
and
day
to
day
imprecision
ranged
from
1.5
to
3.6%
(n
=
20).
These
results
proved
that
the
method
is
more
precise
in
both
within
day
and
day
to
day
assays
and
is
also
highly
reproducible.
Reliability
of
the
proposed
method
was
carried
out
with
QCM
containing
158
mol
L−1of
creatinine.
QCM
was
serially
diluted
for
the
analysis
and
the
measurements
were
carried
out
in
duplicate.
The
calculated
creatinine
concentration
with
respect
to
obtained

322 P.
Nagaraja
et
al.
/
Spectrochimica
Acta
Part
A
92 (2012) 318–
324
Fig.
4.
Analytical
curve
for
the
quantification
of
creatinine
by
the
fixed
time
method.
creatinine
concentration
is
graphically
shown
in
Fig.
5;
the
graph
yielded
y
=
0.998CCr +
0.712
with
linear
regression
coefficient
of
0.999,
the
results
indicated
that
it
is
a
much
reliable
method.
3.5.
Interference
studies
The
extent
of
interference
from
foreign
substances
was
studied
in
3
mL
of
the
solution
containing
55
mol
L−1PPDD,
6
mmol
L−1DMAB
and
53
mol
L−1copper
and
152
mol
L−1fixed
concentration
of
creatinine
in
1
mmol
L−1potassium
dihydrogen
ortho
phosphate/sodium
hydroxide
buffer
at
pH
7.8.
A
deviation
of
±3%
from
the
original
value
in
the
absorbance
reading
was
con-
sidered
tolerable.
The
resultant
tolerance
ratios
are
summarized
in
Table
2.
It
can
be
observed
that
compounds
like
creatine,
glu-
cose,
ammonia,
nitrate,
urea
and
common
inorganic
ions
showed
a
good
tolerance
under
the
given
conditions,
whereas
hemoglobin,
ascorbic
acid,
Fe
(II),
(III),
uric
acid,
nitrite
and
some
drugs
showed
minimum
tolerance
limit.
Table
3
Analytical
recovery
of
creatinine
in
human
urine
samples.
Sample
number
Proposed
method
Standard
method
Creatinine
(mol
L−1)
Added
(mol
L−1)
Found
(mol
L−1)
Recovered
(mol
L−1)
Recovery*
(%)
Creatinine
(mol
L−1)
Added
(mol
L−1)
Found
(mol
L−1)
Recovered
(mol
L−1)
Recovery*
(%)
1
51.2
38
90.3
39.1
102.9
54.9
38
93.6
38.7
101.2
305 366.4
315.2
103.3
305
361.2
306.3
100.4
2
73.3
76
148.2
74.9
98.5
75.0
76
152.1
77.1
101.4
190.6
265.7
192.4
100.9
190.6
267.5
192.5
100.9
3
109.6
38
146.9
37.13
97.8
114.1
38
153.9
39.8
104.7
228.8
344
234.4
102.4
228.8
346.2
232.1
101.8
4
125.53
76
200.9
75.4
99.2
123.9
76
198.1
74.2
97.6
228
355.4
229.9
100.8
228
354.4
230.5
101.1
aMean
of
duplicate
measurement.
*[(Found
creatinine
concentration
−
initial
creatinine
concentration)/added
creatinine
concentration].
Table
4
Analytical
recovery
of
creatinine
in
human
serum
samples.
Sample
number
Proposed
method Standard
method
Creatinine
(mol
L−1)
Added
(mol
L−1)
Found
(mol
L−1)
Recovered
(mol
L−1)
Recovery*
(%)
Creatinine
(mol
L−1)
Added
(mol
L−1)
Found
(mol
L−1)
Recovered
(mol
L−1)
Recovery*
(%)
1
67.18
88.4
157.6
90.42
102.2
61.8
38
99.2
37.4
98.4
265.2
333.32
266.14
100.3
305
366.6
304.8
99.9
2
73.37
88.4
166.97
93.6
105.8
70
76
146.4
76.4
100.5
265.2
344.4
271.03
102.2
190.6
258.4
188.4
98.8
3
90.17
88.4
185.4
95.23
107.8
88.4
38
127.9
39.5
103.4
265.2
357.82
267.65
100.9
228.8
316.5
228.1
99.7
4
122.88
88.4
215.08
92.2
104.3
123.4
76
201.7
78.3
103
265.2
393.38
270.5
101.9
228
352.1
228.7
100.3
aMean
of
duplicate
measurement.
*[(Found
creatinine
concentration
−
initial
creatinine
concentration)/added
creatinine
concentration].
 6
7
6
7
1
/
7
100%