Original Article Survivin -31 G/C polymorphism might contribute to

Int J Clin Exp Med 2015;8(9):15857-15861
www.ijcem.com /ISSN:1940-5901/IJCEM0010983
Original Article
Survivin -31 G/C polymorphism might contribute to
colorectal cancer (CRC) risk: a meta-analysis
Linhua Yao, Yi Hu, Zhongmin Deng, Jingjing Li
Department of Gastroenterology, The First Afliated Hospital of Huzhou Teachers College, 158 Guang Chuang Hou
Lu, Huzhou 313000, Zhejiang, China
Received June 2, 2015; Accepted July 21, 2015; Epub September 15, 2015; Published September 30, 2015
Abstract: Published data has shown inconsistent ndings about the association of survivin -31 G/C polymorphism
with the risk of colorectal cancer (CRC). This meta-analysis quantitatively assesses the results from published stud-
ies to provide a more precise estimate of the association between survivin -31 G/C polymorphism as a possible
predictor of the risk of CRC. We conducted a literature search in the PubMed, Web of Science, and Cochrane Library
databases. Stata 12 software was used to calculate the pooled odds ratios (ORs) with 95% condence intervals
(CIs) based on the available data from each article. Six studies including 1840 cases with CRC and 1804 controls
were included in this study. Survivin -31 G/C polymorphism was associated with a signicantly increased risk of CRC
(OR = 1.78; 95% CI, 1.53-2.07; I2 = 0%). In the race subgroup analysis, both Asians (OR = 1.72; 95% CI, 1.44-2.05;
I2 = 0%) and Caucasians (OR = 1.93; 95% CI, 1.46-2.55; I2 = 0%) with survivin -31 G/C polymorphism had increased
CRC risk. In the subgroup analysis according to site of CRC, survivin -31 G/C polymorphism was not associated with
colon cancer risk (OR = 2.02; 95% CI, 0.79-5.22; I2 = 82%). However, this polymorphism was signicantly associated
with rectum cancer risk (OR = 1.98; 95% CI, 1.42-2.74; I2 = 0%). In the subgroup analysis by clinical stage, both
early stage (I+II) and advanced stage (III+IV) were associated with survivin -31 G/C polymorphism (OR = 1.61; 95%
CI, 1.20-2.16; I2 = 0% and OR = 2.30; 95% CI, 1.70-3.13; I2 = 0%, respectively). In the subgroup analysis by smoke
status, both smokers and non-smokers with survivin -31 G/C polymorphism showed increased CRC risk (OR = 1.47;
95% CI, 1.01-2.13; I2 = 60% and OR = 1.71; 95% CI, 1.28-2.30; I2 = 0%, respectively). In the subgroup analysis by
drink status, both drinkers and non-drinkers with survivin -31 G/C polymorphism showed increased CRC risk (OR =
1.58; 95% CI, 1.06-2.37; I2 = 8% and OR = 1.61; 95% CI, 1.23-2.11; I2 = 0%, respectively). In conclusion, this meta-
analysis suggested that survivin -31 G/C polymorphism may be associated with the risk of CRC
Keywords: Colorectal cancer, survivin, meta-analysis, polymorphism
Introduction
Colorectal cancer (CRC) is one of the most com-
mon malignancies and represents a signicant
cause of morbidity and mortality worldwide [1].
Recent progress in diagnosis and therapy has
helped to save the lives of many patients at
early stages of this malignancy, but the progno-
sis for patients with advanced disease or
metastasis is still poor. Therefore, further
investigation into the molecular pathogenesis
of CRC and the consequential development of
novel targeted therapeutics are needed.
Survivin is a small protein and tumor associat-
ed antigen expressed in many cancers. Survivin
normally functions as an apoptosis inhibitor, via
spindle microtubule and mitotic checkpoint
regulation [2]. It is a potential target for immu-
notherapy since it is highly expressed in many
cancers [3], it is linked to worse prognosis in
both solid and hematologic tumors, and it is
undetectable in almost all normal adult tissues
[4].
Published data has shown inconsistent ndings
about the association of survivin -31 G/C poly-
morphism with the risk of CRC [5-10]. This
meta-analysis quantitatively assesses the
results from published studies to provide a
more precise estimate of the association
between survivin -31 G/C polymorphism as a
possible predictor of the risk of CRC.
Methods
Publication search
We conducted a literature search for relevant
studies on the relationships between survivin
-31 G/C polymorphism and CRC risk in the
PubMed, Web of Science, and Cochrane Library

Survivin and CRC
15858 Int J Clin Exp Med 2015;8(9):15857-15861
databases (up to May 15, 2015). The following
search terms were used: “survivin”; and “Color-
ectal cancer”, and “CRC”. The searched studies
were limited to the English and Chinese.
Inclusion and exclusion criteria
All the studies identied were reviewed inde-
pendently by two investigators and the studies
were included if they fullled the following crite-
ria: (1) a case-control study or cohort study was
reported; (2) the cases were diagnosed as CRC
and the control group was composed of healthy
individuals; (3) the genotypes of survivin -31
G/C polymorphism were described in the stud-
ies. The references were excluded from the
meta-analysis as follows: (1) the study was not
related to CRC; (2) the reference did not
describe genotypes of the survivin -31 G/C
polymorphism in the two groups; (3) the refer-
ence consisted of duplicate data or publica-
tions from the included studies.
Data extraction
The following data were recorded from each
article: rst author, years of publication, ethnic-
ity, gender, age, numbers of subjects, site of
CRC, stage of CRC, smoke and drink status.
The data were extracted by two of the authors
independently. Discrepancies between these
two authors were resolved by discussion.
Statistical analysis
Stata 12 software was used to calculate the
pooled odds ratios (ORs) with 95% condence
intervals (CIs) based on the available data from
each article. P < 0.05 was considered statisti-
cally signicant. The recessive model was esti-
mated. Cochran’s Q-statistic and the I2 test
were used to test the heterogeneity among the
included studies, and P < 0.1 and I2 > 50% sug-
gested signicant differences in study hetero-
geneity. When signicant heterogeneity was
observed across studies, the pooled results
were based on random effects models. The χ2
test was applied to assess whether the geno-
type distributions of the control populations
conformed to Hardy-Weinberg equilibrium
(HWE), and P < 0.05 was considered statisti-
cally signicant. Begg’s funnel plot and Egger’s
test were used to detect publication bias.
Results
Study characteristics
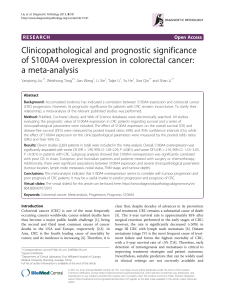
In our study, we initially searched 54 related
references, among which 12 were duplicates.
When removing the duplicates and other unre-
lated references, 6 references met our inclu-
sion criteria and were recruited in the meta-
Figure 1. Flow of study
identication, inclusion,
and exclusion.
Quality assessment
Quality assessment was
conducted for each article
according to Strengthening
the Reporting of Genetic
Association studies (STREGA)
[11] containing eleven items
associated with valid data
reported in the study. For
each item, there are three
degrees, “yes” (scored 2),
“can’t tell” (scored 1) or “no”
(scored 0), after evaluating
each item, a total score from
0 to 22 was reported for each
article. Studies would be
divided into 3 grades: Grade A
(scored 1522, high quality),
Grade B (scored 8-14, medi-
um quality), or Grade C
(scored 0-7, inferior quality).
Only the studies of Grade A or
B would be included in the
nal analysis.

Survivin and CRC
15859 Int J Clin Exp Med 2015;8(9):15857-15861
analysis (Figure 1). The information of the
included studies were listed in Table 1. There
were 2644 subjects, including 1840 cases
with CRC and 1804 controls. All studies
received a score of more than or equal to 17,
indicating good quality.
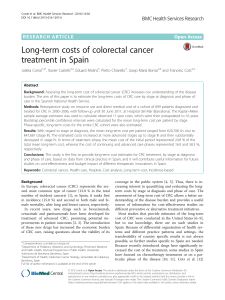
Results of meta-analysis
The results of the association between survivin
-31 G/C polymorphism and CRC risk are sum-
marized in Table 2. Survivin -31 G/C polymor-
phism was associated with a signicantly
increased risk of CRC (OR = 1.78; 95% CI, 1.53-
2.07; I2 = 0%; Figure 2). In the race subgroup
analysis, both Asians (OR = 1.72; 95% CI, 1.44-
2.05; I2 = 0%) and Caucasians (OR = 1.93; 95%
CI, 1.46-2.55; I2 = 0%) with survivin -31 G/C
polymorphism had increased CRC risk. In the
= 8% and OR = 1.61; 95% CI, 1.23-2.11; I2 =
0%, respectively).
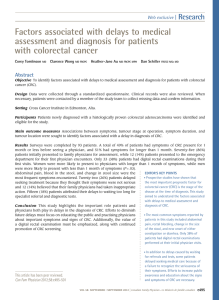
Figure 3 showed the Egger’s publication bias
plot in the meta-analysis. The plots shape, as
well as the P value from Egger’s regression (P =
0.655), did not show evidence of publication
bias.
Discussion
In this meta-analysis, we investigated the asso-
ciation between the survivin -31 G/C polymor-
phism and CRC risk including 1840 cases with
CRC and 1804 controls. We found that individu-
als with survivin -31 G/C polymorphism showed
an increased risk of CRC in the overall popula-
tion. In the stratied analysis by ethnicity, the
signicant association was observed in Asians
Table 1. Characteristics of the studies included in this meta-analysis
Study Year Ethnicity Age
(years)
Gender of
case
No. of
case
No. of
control
Site of
disease
Stage
status
Smoke
status
Drink
status
Quality
grade
Hardy-
Weinberg
equilibrium
Gazouli 2009 Caucasian 33-93 158 men/154 women 312 362 NA Yes NA NA A (scored 21) Yes
Huang 2010 Asian NA 435 men/267 women 702 711 NA NA Yes Yes A (scored 20) Yes
Antonacopoulou 2011 Caucasian 56-86 NA 163 132 NA NA NA NA A (scored 18) Yes
Duan 2012 Asian NA 114 men/92 women 206 129 Yes NA NA NA A (scored 19) Yes
Liu 2012 Asian 25-84 95 men/87 women 182 200 NA NA Yes Yes A (scored 17) Yes
Li 2013 Asian NA 152 men/123 women 275 270 Yes Yes NA NA A (scored 19) Yes
NA, not available.
Table 2. Results of this meta-analysis
Test of association Heterogeneity
OR (95% CI) P Value I2 (%) P Value
Overall 1.78 (1.53-2.07) <0.00001 0 0.68
Ethnicity
Caucasian 1.93 (1.46-2.55) <0.00001 0 0.32
Asian 1.72 (1.44-2.05) <0.00001 0 0.65
Cancer type
Rectum 1.98 (1.42-2.74) <0.0001 0 0.87
Colon 2.02 (0.79-5.22) 0.14 82 0.02
Stage
I+II 1.61 (1.20-2.16) 0.001 0 0.54
III+IV 2.30 (1.70-3.13) <0.00001 0 0.48
Smoking
Yes 1.47 (1.01-2.13) 0.04 60 0.12
No 1.71 (1.28-2.30) 0.0003 0 0.96
Drinking
Yes 1.58 (1.06-2.37) 0.03 8 0.30
No 1.61 (1.23-2.11) 0.0005 0 0.75
subgroup analysis according to site of
CRC, survivin -31 G/C polymorphism was
not associated with colon cancer risk (OR
= 2.02; 95% CI, 0.79-5.22; I2 = 82%).
However, this polymorphism was signi-
cantly associated with rectum cancer
risk (OR = 1.98; 95% CI, 1.42-2.74; I2 =
0%). In the subgroup analysis by clinical
stage, both early stage (I+II) and advan-
ced stage (III+IV) were associated with sur-
vivin -31 G/C polymorphism (OR = 1.61;
95% CI, 1.20-2.16; I2 = 0% and OR = 2.30;
95% CI, 1.70-3.13; I2 = 0%, respectively).
In the subgroup analysis by smoke status,
both smokers and non-smokers with
survivin -31 G/C polymorphism showed
increased CRC risk (OR = 1.47; 95% CI,
1.01-2.13; I2 = 60% and OR = 1.71; 95%
CI, 1.28-2.30; I2 = 0%, respectively). In the
subgroup analysis by drink status, both
drinkers and non-drinkers with survivin
-31 G/C polymorphism showed increased
CRC risk (OR = 1.58; 95% CI, 1.06-2.37; I2

Survivin and CRC
15860 Int J Clin Exp Med 2015;8(9):15857-15861
and Caucasians. In the stratied analysis by
site of CRC, survivin -31 G/C polymorphism sig-
nicantly increased rectum cancer risk, but not
colon cancer risk. We found signicant hetero-
geneity in colon cancer risk. Thus, more studies
with colon cancer risk are still needed. In the
subgroup analysis by stage of CRC, smoking
status and drink status, positive results were
found in all these subgroup analyses.
Kim et al. found that survivin was a candidate
biomarker for the prediction of recurrence and
survival in CRC [12]. Goossens-Beumer et al.
also suggested that identied combined
expression levels of Aldh1, Survivin, and EpCAM
dam et al. observed survivin rs9904341C allele
was associated with increased endometrial
carcinoma risk [18]. Chen and colleagues sug-
gest that the high survivin expression was
associated with tumor stage and grade and
may present a predictive marker of overall sur-
vival in urothelial carcinoma [19].
Some limitations should be addressed. First,
only published English and Chinese language
studies were included in this meta-analysis, so
the language bias might inuence the results.
Second, the sample sizes in several of the
incorporated studies were relatively small,
which may reduce the strength of our conclu-
Figure 3. Funnel plot for the association between survivin -31 G/C polymor-
phism and CRC risk.
as strong independent prog-
nostic factors, with high haz-
ard ratios, for survival and
tumor recurrence in colon
cancer patients [13]. A recent
meta-analysis revealed a pos-
itive correlation between sur-
vivin expression and poor
prognosis in CRC [14]. In addi-
tion, that meta-analysis reve-
aled a signicant association
between expression of sur-
vivin and the presence of
lymph node metastases or
blood vessel invasion [14].
Functionally, survivin exhibits
distinct functions during cell
cycle progression or as inhibi-
tor of programmed cell death
together with IAP-family mem-
ber XIAP, by promoting stabili-
ty of XIAP and synergistically
inhibition of caspase-9 [15].
In addition, survivin promotes
by complexing XIAP invasion
and migration of malignant
cells via NF-κB pathways,
apparently contributing to
metastasis [16].
Surviving also contributed to
other cancers. Javid et al.
demonstrated that survivin
(-31G > C) was associated
with signicantly increased
survivin gene expression and
ultimately may contribute in
the poor clinical outcome of
non-small cell lung cancer
patients [17]. Aminimoghad-
Figure 2. Meta-analysis for the association between survivin -31 G/C poly-
morphism and CRC risk.

Survivin and CRC
15861 Int J Clin Exp Med 2015;8(9):15857-15861
sions. In addition, our result was on the basis of
unadjusted estimates, while a more accurate
analysis should be carried out if more detailed
individual information was available, which
would allow for an adjusted estimate by other
causes such as age and sex.
In conclusion, this meta-analysis suggested
that survivin -31 G/C polymorphism may be
associated with the risk of CRC.
Acknowledgements
This work was supported by Medicine and
health science and technology plan projects in
zhejiang province (2012KYB200) and Huzhou
city technology bureau project (2012 ysb15).
Disclosure of conict of interest
None.
Address correspondence to: Linhua Yao, Depart-
ment of Gastroenterology, The First Afliated
Hospital of Huzhou Teachers College, 158 Guang
Chuang Hou Lu, Huzhou 313000, Zhejiang, China.
Tel: 86-0572-2039425; E-mail: linhuayao11@126.
com
References
[1] Jemal A, Bray F, Center MM, Ferlay J, Ward E,
Forman D. Global cancer statistics. CA Cancer
J Clin 2011; 61: 69-90.
[2] Ambrosini G, Adida C, Altieri DC. A novel anti-
apoptosis gene, survivin, expressed in cancer
and lymphoma. Nat Med 1997; 3: 917-21.
[3] Kawasaki H, Altieri DC, Lu CD, Toyoda M, Tenjo
T, Tanigawa N. Inhibition of apoptosis by sur-
vivin predicts shorter survival rates in colorec-
tal cancer. Cancer Res 1998; 58: 5071-4.
[4] Stauber RH, Mann W, Knauer SK. Nuclear and
cytoplasmic survivin: molecular mechanism,
prognostic, and therapeutic potential. Cancer
Res 2007; 67: 5999-6002.
[5] Gazouli M, Tzanakis N, Rallis G, Theodoropoulos
G, Papaconstantinou I, Kostakis A, Anagnou
NP, Nikiteas N. Survivin -31G/C promoter poly-
morphism and sporadic colorectal cancer. Int J
Colorectal Dis 2009; 24: 145-50.
[6] Huang J, Wang J, Wang L, Liu H, Wei Y, Huang
M. Associationbetween Survivin Promoter
-31C/G Polymorphism and Genetic Suscepti-
bility to Sporadic Colorectal Cancer. J SUN Yat-
sen Univ (Med Sci) 2010; 31: 59-63.
[7] Antonacopoulou AG, Floratou K, Bravou V,
Kottorou A, Dimitrakopoulos FI, Marousi S,
Stavropoulos M, Koutras AK, Scopa CD,
Kalofonos HP. The survivin -31 snp in human
colorectal cancer correlates with survivin
splice variant expression and improved overall
survival. Cell Oncol (Dordr) 2011; 34: 381-91.
[8] Duan F. The Study on the Relationship be-
tween Survivin promoter SNP and the
Colorectal Cancer. Master’s thesis. Lu Zhou
Medical College 2012.
[9] Liu Y. The Association of Survivin Polymorphism
with the Risk of Colorectal Cancer. Master’s
thesis. Hebei Medical College 2012.
[10] Li XB, Li SN, Yang ZH, Cao L, Duan FL, Sun XW.
Polymorphisms of survivinand its protein ex-
pression are associated with colorectal can-
cersusceptibility in Chinese population. DNA
Cell Biol 2013; 32: 236-42.
[11] Little J, Bradley L, Bray MS, Clyne M, Dorman J,
Ellsworth DL, Hanson J, Khoury M, Lau J,
O’Brien TR, Rothman N, Stroup D, Taioli E,
Thomas D, Vainio H, Wacholder S, Weinberg C.
Reporting, appraising, and integrating data on
genotype prevalence and gene-disease asso-
ciations. Am J Epidemiol 2002; 156: 300-10.
[12] Kim ST, Sohn I, DO IG, Jang J, Kim SH, Jung IH,
Park JO, Park YS, Talasaz A, Lee J, Kim HC.
Transcriptome analysis of CD133-positive
stem cells and prognostic value of survivin in
colorectal cancer. Cancer Genomics Proteo-
mics 2014; 11: 259-66.
[13] Goossens-Beumer IJ, Zeestraten EC, Benard A,
Christen T, Reimers MS, Keijzer R, Sier CF,
Liefers GJ, Morreau H, Putter H, Vahrmeijer AL,
van de Velde CJ, Kuppen PJ. Clinical prognostic
value of combined analysis of Aldh1, Survivin,
and EpCAM expression in colorectal cancer. Br
J Cancer 2014; 110: 2935-44.
[14] Krieg A, Werner TA, Verde PE, Stoecklein NH,
Knoefel WT. Prognostic and clinicopathological
signicance of survivin in colorectal cancer: a
meta-analysis. PLoS One 2013; 8: e65338.
[15] Dohi T, Okada K, Xia F, Wilford CE, Samuel T,
Welsh K, Marusawa H, Zou H, Armstrong R,
Matsuzawa S, Salvesen GS, Reed JC, Altieri
DC. An IAP-IAP complex inhibits apoptosis. J
Biol Chem 2004; 279: 34087-90.
[16] Mehrotra S, Languino LR, Raskett CM,
Mercurio AM, Dohi T, Altieri DC. IAP regulation
of metastasis. Cancer Cell 2010; 17: 53-64.
[17] Javid J, Mir R, Julka PK, Ray PC, Saxena A. Role
of survivin re-expression in the development
and progression of non-small cell lung cancer.
Tumour Biol 2015; 36: 5543-50.
[18] Aminimoghaddam S, Shahrabi-Farahani M,
Mohajeri-Tehrani M, Amiri P, Fereidooni F,
Larijani B, Shaee G, Amoli MM. Epistatic inter-
action between adiponectin and survivin gene
polymorphisms in endometrial carcinoma.
Pathol Res Pract 2015; 211: 293-7.
[19] Chen HA, Su CM, Hsieh HY, Tung CL, Hsu CD,
Wang YH, Shen CH. Clinical signicance of sur-
vivin expression in patients with urothelial car-
cinoma. Dis Markers 2014; 2014: 57498.
1
/
5
100%